
To answer questions on what services and barriers people with psychiatric disorders face, the authors conducted two targeted literature reviews: (1) employment programs and outcomes for people with psychiatric disorders; and (2) employment programs for people with other disabilities. Also analyzed was data from the Survey of Income and Program Participation to examine service-use trajectories of vulnerable populations that might be expected to apply for Social Security Disability Insurance benefits. The authors also examined literature and policy documents that outlined funding options for employment services for people with psychiatric disorders and other disabilities.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
"Acronyms
The following acronyms are mentioned in this report and/or appendices.
| AB | Accelerated Benefits |
|---|---|
| ACA | Affordable Care Act also known as the Patient Protection and Affordable Care Act |
| ACO | Accountable Care Organization |
| ACT | Assertive Community Treatment |
| ADA | Americans with Disabilities Act |
| ADL | Activity of Daily Living |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| ASD | Autism Spectrum Disorder |
| C | Control (group) |
| CBT | Cognitive Behavioral Therapy |
| CI | Confidence Interval |
| CMHS | Community Mental Health Services |
| CMS | HHS Centers for Medicare and Medicaid Services |
| DM | Disability Management |
| DMIE | Demonstration to Maintain Independence and Employment |
| DRA | Deficit Reduction Act |
| DSM | Diagnostic and Statistical Manual |
| e.s. | Effect Size |
| EBD | Emotional/Behavioral Disturbance |
| EDIPP | Early Detection, Intervention, and Prevention of Psychosis Program |
| EHB | Essential Health Benefits |
| EI | Early Intervention |
| EIDP | Employment Intervention Demonstration Program |
| EN | Employment Network |
| FACT | Family-Aided Assertive Community Treatment |
| FE | First Episode |
| FPL | Federal Poverty Level |
| FT | Full-Time |
| GED | General Equivalency Diploma |
| HCBS | Home and Community-Based Services |
| HHS | U.S. Department of Health and Human Services |
| HMO | Health Maintenance Organization |
| HS | High School |
| HWVP | Homeless Women Veteran Program |
| IDA | Individual Development Account |
| IEP | Individualized Education Program |
| IMD | Institution for Mental Disease |
| IPS | Individual Placement and Support |
| LA | Los Angeles |
| LBP | Low Back Pain |
| LR | Literature Review |
| MCS | Mental Component Summary |
| MFP | Money Follows the Person |
| MHPAEA | Mental Health Parity and Addiction Equity Act |
| MHTS | Mental Health Treatment Study |
| MS | Multiple Sclerosis |
| n.s. | Not Sigificant |
| N/A | Not Applicable |
| ND | No Data |
| NSR | Non-Systematic Review |
| OECD | Organisation for Economic Co-operation and Development |
| OR | Odds Ratio |
| OS | Observational Study |
| PGAP | Progressive Goal Attainment Program |
| PT | Part-Time |
| PTSD | Post-Traumatic Stress Disorder |
| QALY | Quality Adjusted Life Years |
| QED | Quasi-Experimental Design |
| RAISE | Recovery After an Initial Schizophrenia Episode |
| RCT | Randomized Controlled Trial |
| RSA | Rehabilitation Services Administration |
| RTW | Return-to-Work |
| SAMHSA | HHS Substance Abuse and Mental Health Services Administration |
| SE | Supported Employment |
| SIPP | Survey of Income and Program Participation |
| SMI | Serious Mental Illness |
| SNAP | Supplemental Nutrition Assistance Program |
| SR | Systematic Review |
| SSA | U.S. Social Security Administration |
| SSDI | Social Security Disability Insurance |
| SSI | Supplemental Security Income |
| SSN | Social Security Number |
| STETS | Structured Training and Employment Transition Services |
| T | Treatment (group) |
| TANF | Temporary Assistance for Needy Families |
| TAY | Transition-Age Youth |
| TCM | Targeted Case Management |
| TETD | Transitional Training Employment Demonstration |
| TIP | Transition to Independence Process |
| TTW | Ticket to Work |
| VA | Veterans' Affairs |
| VR | Vocational Rehabilitation |
| VR&E | Vocation Rehabilitation and Employment |
| WPDM | Workplace Disability Management |
| YTD | Youth Transition Demonstration |
Executive Summary
Introduction
The Office of the Assistant Secretary for Planning and Evaluation (ASPE) in the U.S. Department of Health and Human Services funded the Improving Employment Outcomes for People with Psychiatric Disorders and Other Disabilities Project to identify effective programs that help individuals with psychiatric disorders find and retain employment. A second goal of the project was to explore how these programs can be funded through the Affordable Care Act (ACA) and other sources. ASPE was particularly interested in knowing what supports will assist the following subgroups of people with psychiatric disorders:
-
Individuals who are now or who are expected to be long-term clients of mental health services and who are in the process of applying for disability benefits.
-
Individuals at risk of losing employment due to mental illness.
-
Individuals, such as transition-age youth (TAY), who are experiencing an initial episode of psychosis and require early-intervention (EI) services.
This project aimed to find answers to the following overarching questions:
-
What services are most effective at helping people in the previously described three subgroups find and keep employment?
-
What are the work-support needs of and services currently available to individuals with other disabilities? What can income and service-use trajectories of participants in particular programs tell us about service needs and program effectiveness?
-
What policies and funding can be adopted in a post-ACA environment to overcome employment barriers for people with psychiatric disorders and other disabilities?
We conducted two targeted literature reviews: (1) employment programs and outcomes for people with psychiatric disorders (O'Day et al. 2013); and (2) employment programs and outcomes for people with other disabilities (Martin et al. 2013). We also analyzed data from the Survey of Income and Program Participation to examine service-use trajectories of vulnerable populations who might be expected to apply for Social Security Disability Insurance (SSDI) benefits. We also examined literature and policy documents that outlined funding options for employment services for people with psychiatric disorders and other disabilities. We highlight our findings in this summary.
Evidence for Improving Employment Outcomes for Individuals with Psychiatric Disorders
A number of employment programs and services have proven effective at helping people with serious mental illness (SMI) and other psychiatric disorders find and keep work. In particular, evidence-based supported employment (SE), especially the standardized Individual Placement and Support model, has been shown to be more effective than traditional vocational programs in helping people with SMI obtain competitive employment. SE is a strategy for helping people with disabilities participate in the labor market, in a job of their choosing, with professional support (Bond et al. 2001). SE helps individuals with a variety of characteristics--age, gender, diagnosis, education, and so on--achieve higher rates of competitive employment than those in control-groups who have the same characteristics. Job-development services and integration of vocational and clinical services are vital for making SE successful. However, room for improvement remains. Those who received SE and obtained employment found only part-time jobs with low wages, and we found little strong evidence for positive long-term outcomes. The absence of improved long-term outcomes may result from the lack of programmatic emphasis on job tenure and economic self-sufficiency, or work disincentives built into Social Security disability and other financial-support programs that discourage more than minimal levels of work.
Several strategies have been used to improve employment outcomes for individuals who are now or who are expected to be long-term clients of traditional mental health services and may be in the process of applying for disability benefits. Although it is difficult to identify this subgroup of people with SMI before they become attached to the Social Security disability benefits and mental health systems, the population is of interest to policymakers because once they begin receiving benefits, the likelihood of their returning to work is minimal (Social Security Administration [SSA] 2011a, 2011b). The Accelerated Benefits Demonstration, funded by the SSA, showed that providing vocational and other support services along with health insurance may lead to improved short-term employment outcomes for new SSDI beneficiaries with mental health impairments. There is limited evidence that providing SE along with housing supports may improve employment outcomes for people with SMI who are homeless, and that SE may improve employment outcomes for veterans with SMI. More research is needed to establish a strong evidence base for the effectiveness of these services, as well as for services to other discrete populations of people with SMI, such as ex-offenders or recipients of Temporary Assistance for Needy Families.
The occupational outcomes of interventions for workers with mental illnesses at risk of job loss are not as well established. Few high quality studies of the impact of interventions on the employment of workers with mental illness exist. However, two sites from the Demonstration to Maintain Independence and Employment suggest that providing "wrap-around" health services to people with SMI may increase earnings and decrease reliance on federal disability benefits. Several other studies offer hope that employer interventions, such as depression screening, EI, and providing reasonable accommodations, increase job tenure and hours worked, and reduce job loss for workers with mental illness; for example, Wang et al. (2007) demonstrated that a telephone-based care management program targeted to employees with significant depression significantly improved job retention and hours worked.
Some well-established EI programs provide services to people who experience a first episode of mental illness. Evidence suggests that intervening early may help prevent full-blown psychosis and long-term involvement with the mental health and disability systems, especially when the intervention includes an SE component. Evidence of the efficacy of these programs for people with schizophrenia is limited but positive. Studies of the effects on employment outcomes of services for a broader range of TAY are few, but it appears that services may be more effective for older than for younger individuals in this category. Work in this field continues to be an important priority for researchers and policymakers. Several studies are underway that should offer more evidence in the future on the effectiveness of services for this population.
Several other innovative approaches to employing people with psychiatric disabilities have been discussed in the literature. More research is needed to establish the effectiveness for individuals with psychiatric disorders of self-employment and consumer-managed firms, asset-development, financial-literacy programs, and self-determination models. The evidence for social enterprises, consumer-provided services, and supported education is more substantial, but more work must be done to establish which models are most effective and how much to expect from them.
Evidence for Return-to-Work and Employment-Support Programs for People with Other Disabilities
We also reviewed literature on return-to-work (RTW) and employment-support programs for people with other disabilities, including physical, intellectual, and sensory. We reviewed evidence from programs sponsored by employers, demonstrations sponsored by the Federal Government, and employment interventions in other countries.
Most of the evidence of success with EI services is based on employer-sponsored RTW and employment supports, also known as disability management (DM), delivered to workers on sick leave or before employment is terminated. In general, these reviews show that employer-sponsored RTW components, such as workplace accommodations, RTW coordinators, contact between a health care provider and the workplace, and modified job duties or work schedules are effective in retaining employees with general health conditions who otherwise would exit jobs for health or disability reasons. Most of the evidence of DM success pertains to persons with musculoskeletal disorders--a broad category of conditions that may include injury or damage to, or disorders of the joints or other tissues in the upper or lower limbs or back. We identified relatively few high quality systematic reviews of RTW or employment-support interventions focused on other specific disabilities or impairments, making it imprudent to draw conclusions about their findings.
We found a little evidence on the effectiveness of RTW programs for veterans, and a lack of rigorous high quality evidence supporting state and federal vocational rehabilitation (VR). We identified two reports summarizing evaluations of federally funded interventions directed at individuals who are unemployed and Social Security disability program beneficiaries. The results of these interventions indicate that more intensive interventions with individualized supports can produce impacts on employment and earnings than less intensive interventions.
We identified several systematic reviews that were international in scope or included United States and non-United States studies. These reviews also indicate moderate evidence of success for DM interventions, including RTW coordinators; however, it is not readily apparent whether reviews that focus primarily on non-United States countries can be generalized to United States settings.
Pre-Application Work Activity of SSDI Applicants
We examined the employment and program-participation paths of individuals with disabilities who did and did not apply for SSDI. The patterns help us understand the characteristics of those at greater risk of SSDI entry compared to those who do not enter SSDI, most of whom continued working. This can help craft policies that simultaneously divert those with disabilities from applying for SSDI while providing the support necessary to make work feasible for those with disabilities.
As expected, we observed a decline in employment and earned income of SSDI applicants before applying for benefits, with the biggest change observed in the six months immediately preceding SSDI application. However, somewhat surprisingly, a large share of these individuals (more than two-thirds) were employed during this period and over half were covered by private insurance with Medicaid covering most of the rest. This may suggest an opportunity to divert SSDI entry by providing employment supports to maintain connection to the workforce.
A significant proportion of eventual SSDI applicants received some type of poverty-related benefit up to 42 months before applying for SSDI, and participation in these benefits programs showed an increase during the six months immediately before SSDI application. Among individuals in at-risk groups, those with private disability insurance had the highest rates of applying for SSDI. Participation in income and other support programs increased markedly during the six months before SSDI application. This increased access to some benefit programs--most notably, employer-based disability insurance, workers' compensation, Supplemental Nutrition Assistance Program, and Medicaid--may point to areas where investments in EI initiatives could be fruitful.
Funding for Employment Services and Supports for People with Psychiatric Disorders and Other Disabilities
Several mechanisms exist to fund employment supports for people with psychiatric disorders and other disabilities, but the funding picture is imperfect. Medicaid provides several options, such as the 1915(c) Home and Community-Based Services waiver, state plan options, the managed care delivery system waiver, and the Medicaid rehabilitation services option. However, individuals must meet very specific eligibility requirements to receive them. States have cobbled together funding from various Medicaid provisions, their own state VR agencies, and grants from Substance Abuse and Mental Health Services Administration and other sources, but many people find it difficult or impossible to access SE and other employment services. The mechanisms most commonly used to fund SE services are typically available only to people who have already been identified as disabled and are most often already receiving Social Security disability benefits. Their availability for populations not yet dependent on benefits is often limited.
Elements of the ACA that Might Affect Individuals with Psychiatric Disorders and Other Disabilities
The ACA can serve as a means to expand current payment options for DM, SE, and other employment supports. This important new law contains several provisions that have the potential to positively impact individuals with mental illness and to lessen the degree to which a lack of health care coverage may incentivize people to seek public benefits. These provisions include the Medicaid expansion and the introduction of the state-based health insurance exchanges, the establishment of mental health and substance use disorder services as "essential health benefits," and coverage up to age 26 on a parent's plan. Because these provisions have the potential to expand access to coverage, the ACA is a significant step toward breaking the link between eligibility for Social Security disability benefits and public health insurance. This step may weaken the incentive to forego employment and remain on Social Security disability benefits in order to maintain health care benefits. Similarly, because the ACA extends medical coverage to those who heretofore have been ineligible for or unable to purchase coverage, it also has the potential to increase access to employment services and supports in a number of ways.
In January 2014, provisions of the ACA that allow states to expand their Medicaid programs went into effect. In states that accept this option, low-income and moderate-income residents who do not meet the definition of disability for Supplemental Security Income or SSDI or are otherwise ineligible for Medicaid are able to obtain health care coverage. Other reforms to the private health insurance market are also likely to increase access to health insurance and services for people with mental illnesses and other disabilities.
Conclusion
In conclusion, our literature review found that evidence-based SE provides the strongest evidence for helping people with SMI to find work, but there is little strong evidence for positive long-term outcomes. The absence of improved long-term outcomes may result from work disincentives built into Social Security disability and Medicaid programs that discourage more than minimal levels of work, or from lack of long-term funding options for SE. The ACA may provide a better source of long-term funding, since it expands the population of individuals eligible for Medicaid and offers additional options for health insurance coverage.
The ACA may support workers by expanding eligibility for health insurance among low-income people who experience SMI and among individuals who experience a psychiatric disorder that does not qualify them for Social Security disability benefits. Evidence suggests that intervening early may help prevent full-blown psychosis and long-term involvement with the mental health and disability systems, especially when the intervention includes an SE component. Because the ACA enables youth to remain on their parents' insurance until age 26, mental health services and supports may become more available to this population. The ACA could also improve availability of vocational and other support services along with health care coverage for low-income populations leading to improved employment outcomes for this group and perhaps fewer applications for SSDI.
Our analysis shows a consistent decline in employment as early as three years before SSDI receipt. Targeting individuals who leave employment due to a mental illness and go on to apply for means-tested benefits or private disability insurance, or those with high health expenditures or those receiving workers' compensation benefits may reduce future applications for SSDI.
I. Introduction
A. Background
Less than 20 percent of people who receive publicly funded mental health services are employed, yet less than 2 percent receive evidence-based supported employment (SE) services that might improve their employment prospects (Substance Abuse and Mental Health Services Administration [SAMHSA] 2011). Research consistently demonstrates that, with the right supports, 40-60 percent of people with serious mental illness (SMI) can work, although many work part-time, intermittently, or at low wages (Blyler 2003; Bond 2004, 2007; SAMHSA 2011). Unemployment or low levels of work may lead to reliance on disability benefit programs, which gives the social safety-net an important role in their lives.
Individuals who are unable to work because of psychiatric disorders often turn to publicly funded income support and health insurance programs to survive. Sixty-four percent of those receiving publicly funded mental health services receive Medicaid (SAMHSA 2011). Working-age people with psychiatric disorders are the largest and most rapidly expanding group of Social Security Disability Insurance (SSDI) and Supplemental Security Income (SSI) beneficiaries. Currently, 36 percent of SSDI and 60 percent of working-age SSI beneficiaries have a mental illness (Social Security Administration [SSA] 2011a, 2011b), and estimates suggest that less than 4 percent of SSDI beneficiaries exit the program due to earnings within the first ten years of enrollment (Stapleton et al. 2010). Estimates of the direct costs of providing SSDI and SSI for people with SMI and the lost earnings resulting from unemployment exceed $217 billion annually (Insel 2008).
A lack of health insurance and access to affordable health care may contribute to low employment rates among people with psychiatric disorders and other disabilities. Individuals who do not have access to insurance through a family member may lack health insurance if they do not work, work in a job that does not offer health benefits, or cannot afford to pay the premiums associated with the plan offered by their employer. Without access to health insurance, people may not be able to afford the treatment needed to improve or maintain their mental health sufficiently to allow them to work. The need for health insurance, therefore, can be a powerful incentive for uninsured people experiencing persistent mental health problems or other disabling conditions to apply for SSI or SSDI to obtain Medicare and/or Medicaid coverage, even if they would otherwise be able to work (Maestas 2012).
Limited access to affordable health care has been a particular barrier for people with psychiatric disorders because of the historical lack of parity between insurance coverage of mental health and other types of health care. In the SAMHSA Employment Intervention Demonstration Program (EIDP), a multisite research study investigating the effectiveness of SE for improving employment among adults with SMI, only 24 percent of full-time jobs obtained by treatment-group members included medical benefits, and even fewer covered mental health care (Cook et al. 2006). Before the Affordable Care Act (ACA), young people who experienced serious mental health challenges for the first time as adults were especially vulnerable to being uninsured when they aged out of their parents' coverage but were not yet employed in jobs that provided health benefits.
The ACA, which was implemented in January 2014, has the potential to mitigate employment barriers resulting from the lack of affordable health care. Relevant provisions include prohibitions on denying coverage based on pre-existing mental health conditions and on annual and lifetime coverage limits, extended Medicaid eligibility to working-age adults with income of up to 138 percent of the federal poverty level (FPL), and subsidies to people with incomes up to 400 percent of the FPL to purchase health insurance from state health exchanges (Rosenbaum et al. 2011; Levy et al. 2012). The ACA also expands the federal mental health parity requirements (Sarata 2011) and mandates coverage of mental health and substance use disorder services among individual, small-group, and Medicaid health insurance plans (Centers for Medicare & Medicaid Services [CMS] 2011). With improved access to affordable health insurance under the ACA, consumers may no longer have to rely solely on SSDI and SSI to obtain needed health care. With the link between SSI and SSDI participation and access to public health insurance removed, people with SMI will be more able to work without fear of risking their mental health due to a lack of health insurance.
B. Purpose of the Report
The Office of the Assistant Secretary for Planning and Evaluation (ASPE) in the U.S. Department of Health and Human Services (HHS) funded the Improving Employment Outcomes for People with Psychiatric Disorders and Other Disabilities Project. The purpose of this project is to identify policy measures that are barriers or facilitators to employment among people with psychiatric disorders and identify improvements in health care and human services programs in a post-ACA environment that are likely to reduce these barriers. ASPE was particularly interested in knowing what supports will assist the following subgroups of people with psychiatric disorders:
-
Individuals who are now or who are expected to be long-term clients of mental health services and are in the process of applying for disability benefits.
-
Individuals at risk of losing employment due to mental illness.
-
Individuals experiencing an initial episode of psychosis and needing early-intervention (EI) services, such as transition-aged youth.
ASPE also wished to explore how the ACA can be used to fund services and supports that will assist people with SMI who are in the aforementioned three subgroups to find and keep employment.
This project targeted the following overarching questions:
-
What services are most effective in helping people with psychiatric disorders in the three subgroups mentioned above find and keep employment?
-
What are the work-support needs of and services currently available to individuals with other disabilities? What can income and service-use trajectories of participants in particular programs tell us about service needs and program effectiveness?
-
What policies and funding can be adopted to overcome employment barriers for people with psychiatric disorders and other disabilities in a post-ACA environment?
To answer these questions, we conducted two targeted literature reviews: (1) employmentprograms and outcomes for people with psychiatric disorders (O'Day et al. 2013); and (2) employment programs for people with other disabilities (Martin et al. 2013). We also analyzed data from the Survey of Income and Program Participation (SIPP) to examine service-use trajectories of vulnerable populations that might be expected to apply for SSDI benefits. We also examined literature and policy documents that outlined funding options for employment services for people with psychiatric disorders and other disabilities.
C. Organization of the Report
The remainder of the report is organized as follows. In Chapter II, we summarize the findings of a systematic review of evidence on employment services and supports provided to people with SMI in the three subgroups mentioned above. In Chapter III, we synthesize evidence on the effectiveness of work supports and services currently available to the broader population of people with disabilities. In these two chapters, we summarize the significant findings of more extensive literature reviews we previously prepared for ASPE. In Chapter IV, we describe the employment and program-participation patterns of people with disabilities before they apply for SSDI. We synthesize existing data to produce statistics on the characteristics of subgroups of people with disabilities and their disability, work, and service-use trajectories. In Chapter V, we describe the funding mechanisms that can be used to pay for the services described in Chapter II and Chapter III. In the final chapter, we summarize the previous chapters and provide an analysis of opportunities and barriers to employment in the post-ACA environment.
Four appendices provide further details about the literature review methods and the SIPP analysis. We present tables summarizing the studies we reviewed in Appendix A and our overall methodology for conducting the literature reviews in Appendix B. Appendix C provides details about the methods for the SIPP analysis and Appendix D provides additional tables.
II. Evidence for Improving Employment Outcomes for Individuals with Psychiatric Disorders
A. Introduction
In this chapter, we consider the evidence for improving employment outcomes for people with psychiatric disorders, to provide background for our discussion of the three targeted subgroups of people with SMI we consider in later sections of this chapter. We begin by describing the evidence on SE services for people with psychiatric disabilities in general and continue by examining evidence for SE and other services in the three study target groups (See Appendix A, for summaries of the studies we reviewed). In Section B, we describe the components of SE and Individual Placement and Support (IPS), a standardized SE model, as well as efforts to enhance and increase access to SE. We then review the existing evidence for improving employment outcomes through SE programs in Section C. In Section D, Section E, and Section F, we consider evidence on employment services for individuals who are now or who are expected to be long-term recipients of mental health services but who do not yet receive disability benefits, workers at risk of job loss due to mental illness, and individuals who experience a first episode (FE) of psychosis, including transition-age youth (TAY). In Section G, we briefly review evidence on other services that might have an impact on employment outcomes.
B. Supported Employment
SE is a strategy for helping people with disabilities participate in the labor market, in a job of their choosing, with professional support (Bond et al. 2001). The term "evidence-based SE" has been coined to refer specifically to the types of SE services that adhere to the full set of specific evidence-based principles, including: (1) a focus on obtaining competitive employment in the community; (2) rapid job search; (3) integration of mental health and employment services; (4) emphasis on client preferences during the job search; (5) ongoing, time-unlimited individualized support after job placement; and (6) personalized benefits counseling (Bond 2004, 2008; Twamley et al. 2003).1
After learning that SE services were not widely available despite evidence of the model's effectiveness, the Dartmouth Psychiatric Research Center worked with Johnson & Johnson to form a public/private partnership to train state staffs and provide technical assistance to help states implement and expand the standardized form of evidence-based SE. The collaborative seeks to overcome a common challenge--disparate organizational structures and funding streams between mental health and vocational rehabilitation (VR) systems--that make it difficult to implement IPS (Drake et al. 2006). By January 2013, the program had expanded to 12 states, the District of Columbia, and Alameda County, California. From July 2012 through September 2012, 10,474 people received IPS services from the participating states, and 41 percent of them worked in competitive jobs.2
C. Evidence for Improving Employment Outcomes through Supported Employment
1. There is strong evidence that SE is more effective in helping people with SMI obtain competitive employment than traditional vocational programs. Yet, even with SE, about half of participants did not find competitive work. For those that did, jobs were part-time and of short duration, and earnings were low.
We reviewed reports on 18 randomized controlled trials (RCTs) of SE services (Appendix A, Table A.1 and Table A.2). Sixteen of these studies reported competitive employment rates, defined as working at a competitive job at any time during the study period. In 11 of them, competitive employment rates were significantly higher in the SE groups than in the control-groups. Overall, 27-78 percent of SE participants found competitive employment, compared with 7-40 percent of control participants. Across the high-fidelity SE studies reviewed in Bond et al. (2008), competitive employment rates were 61 percent, on average, among SE participants, compared with 23 percent among controls. Cross-site evaluations of EIDP also found that, compared with those who receive services-as-usual or weaker forms of the intervention, SE recipients were significantly more likely to achieve competitive employment (55 percent versus 34 percent). Employment rates increased over the course of the 24-month study period (Cook et al. 2005b).
Job duration across these studies appears to be short, with participants staying in a given job for an average of only 14-21 percent of the study duration (Twamley et al. 2003), but the durations of most of these studies were two years or less. Employment outcomes are likely to improve over time as participants adjust to work environments and gain work experience. In addition, longer-term program interventions targeting wages and job tenure to the same degree as initial attainment of competitive employment might have led to more positive results.
Part-time work is the norm for both SE and traditional employment programs. Research suggests SE participants work more and earn more, but the evidence is slim. Across EIDP sites, SE recipients were significantly more likely than controls to work 40 or more hours per month (51 percent versus 39 percent) (Cook et al. 2005b). Among participants in the Mental Health Treatment Study (MHTS) who obtained at least one competitive job, both treatment and control-group members worked about 20 hours per week and earned only about $200 per week at the job they held the longest or at which they worked the most hours (Frey et al. 2011).
2. Participants with a variety of characteristics benefit from SE.
Two studies found that SE was more effective than control interventions regardless of the participants' demographic and background characteristics. Frey et al. (2011) analyzed employment for MHTS participants by age, gender, diagnosis, and education. The SE group had significantly higher competitive employment rates than controls in every category. In EIDP, although certain individual characteristics were associated with poorer employment outcomes overall, employment outcomes for people with such characteristics improved significantly with receipt of SE service. For example, although study participants with schizophrenia or who lived in localities with a high unemployment rate had poorer employment outcomes overall, Cook et al. (2006, 2008) found a greater effect of SE for these groups than for those with other diagnoses or living in areas with lower unemployment rates; these results suggest that SE may be particularly effective at ameliorating factors that otherwise serve as barriers to employment.
3. Job-development services and strong integration of vocational and clinical services are key components of SE.
Understanding which specific elements of SE are important for vocational success is vital for replicating and improving SE models. As reported in Cook et al. (2005b), EIDP found that individuals receiving job-development services--defined as tailored job-seeking activities to match jobs to clients--were nearly five times more likely to obtain a competitive position. Without job-development services, participants were very unlikely to gain competitive employment, especially if they had no prior work experience. Notably, ongoing job support was not associated with the total number of hours worked but was associated with significantly longer tenure for a first competitive job. Another analysis of EIDP data found that those receiving services from SE programs with high degrees of integration were over 2.5 times more likely to be competitively employed and nearly twice as likely to work 40 or more hours per month (Cook et al. 2005b). Receiving more hours of vocational services was associated with better employment outcomes, whereas receiving more hours of clinical services was negatively associated with employment outcomes, even when controlling for work history, diagnosis, level of functioning, and receipt of SSA disability benefits.
In sum, there is evidence for the effectiveness of SE, but room for improvement remains. The lack of strong evidence for long-term outcomes may result from the lack of programmatic emphasis on job tenure and economic self-sufficiency. Work disincentives built into Social Security disability and other financial-support programs may also contribute to lower work and earnings levels.
D. Services for People Who Are Now or Who Are Expected to Be Long-Term Clients of Mental Health Services
In this section, we review the literature on services and interventions for people who are now or who are expected to be long-term clients of traditional mental health services and who are in the process of applying for SSDI or SSI (Appendix A, Table A.3). Because these individuals have not been studied as a group, we considered research on specific subpopulations likely to comprise such individuals, including new SSDI beneficiaries and people who are homeless, military veterans, and ex-offenders with SMI who may eventually turn to disability benefits for support.
1. Vocational and other support services provided along with health insurance may lead to improved short-term employment outcomes for new SSDI beneficiaries with mental health impairments. Providing health insurance alone had no impact.
The Accelerated Benefits (AB) demonstration project, funded by SSA, was designed primarily to test the effects of providing health insurance to new SSDI beneficiaries without having to wait the required 24 months before becoming eligible for Medicare. We include this study because the circumstances of new SSDI beneficiaries, particularly those without health care, might be similar to applicants for SSDI benefits. Demonstration participants were randomly assigned into a AB group who received health insurance (N=400); an AB Plus group who received health insurance as well as medical case management, employment and benefits counseling services, and Progressive Goal Attainment Program3 services (N=611); and a control-group (N=983). The AB Plus group participated in employment or VR services at a significantly greater rate (p=.005) at one and two years after random assignment than either the AB group or the control-group. The AB Plus program led to a 5.3 percentage point, or nearly a 50 percent increase, in employment and to an $831 increase in annual earnings in the second calendar year following enrollment. Access to health care plus vocational and support services were necessary to produce these results.
These positive effects disappear in Year 3, either due to SSA work disincentives (the timing is consistent with the loss of SSDI cash benefits due to work activity), the end of program services, or worsening of beneficiaries' health condition (Michalopoulous 2011; Stegman & Weathers 2013). Findings for the 22 percent of the study sample with mental health impairments mirror this pattern.
2. Limited evidence suggests that providing SE along with housing supports may improve employment outcomes for people with SMI who are homeless.
We identified three promising approaches that assist people with SMI who are homeless to find employment. The most rigorously evaluated of these, Los Angeles' (LA's) HOPE, provided SE, supportive housing, and direct payment for such items as vocational classes, work clothing, and equipment to people with SMI who were formerly homeless. LA County designated three of its 18 programs that provide supportive services and housing assistance to homeless individuals with SMI as LA's HOPE sites. The overall employment rate for LA's HOPE clients was more than double that of the comparison group who received housing services at other sites (57 percent versus 22 percent), as was the competitive employment rate (27 percent versus 13 percent) (Burt 2012).
3. Limited evidence suggests that evidence-based SE may be effective for veterans with SMI.
A recent systematic review suggests limited knowledge of how to reintegrate veterans with mental disorders into a new workplace after an absence of more than a year (Vantil et al. 2012). Of the 97 studies of programs for people with mental disorders reviewed, ten were studies of veterans. The review concluded that although the evidence-based model of SE has the strongest evidence base for facilitating workplace reintegration for individuals with SMI, the literature dealing with reintegration, especially for veterans, is sparse.
The most promising study included in the review was a RTC focused on veterans with post-traumatic stress disorder (PTSD) conducted at the Tuscaloosa Veterans Affairs (VA) Medical Center between 2006 and 2010 (Davis et al. 2012). Eighty-five veterans with PTSD were randomly assigned to receive either SE services or the standard VA VR Program, which provided work therapy through set-aside temporary jobs. Veterans in the SE group were significantly more likely to gain competitive employment, competitive employment more quickly, work in a competitive job more weeks, and earn higher wages.
A study of SE for homeless veterans with psychiatric or addiction disorders, not covered in the systematic review, showed similar results (Rosenheck & Mares 2007). The intervention tested a low-intensity teleconference training approach (average cost of $6,033 per site) for implementing the SE model at nine VA programs and compared outcomes before and after implementation. The post-implementation group of veterans engaged in significantly more days of competitive employment, higher levels of competitive employment, and earned higher wages than the pre-implementation group over the two-year follow-up period.
4. We found no studies examining the effectiveness of employment interventions for ex-offenders.
Individuals with SMI are overrepresented in the criminal justice system (Schnittker et al. 2011), and having a criminal record presents additional challenges for finding employment upon release from jail or prison. Without supports to aid in overcoming these challenges, ex-offenders with SMI may seek SSI or SSDI as a source of income support and a route to health insurance. Promising efforts are demonstrating the effectiveness of cooperation between the criminal justice and mental health systems to provide services to individuals with SMI upon their release. These efforts involve cognitive behavioral therapy, case management, medication and substance abuse monitoring, and referral to community agencies (Osher et al. 2012). Consistent with the findings of Anthony (2006) and Osher & Steadman (2007), however, we were not able to identify any published studies regarding the effective employment supports for this population.
E. Employment Interventions for Workers with Serious Mental Illness At-Risk of Job Loss
In this section, we summarize findings on the current state of knowledge on interventions to improve employment outcomes among workers with mental illness at risk of job loss. Following a framework established by Nieuwenhuijsen et al. (2008) and Krupa (2007), our review divides interventions into two main groups: individual or worker level interventions and employer-level interventions. Individual-level interventions are typically directed to the worker, such as EI, assessment, counseling, coping skills training, return-to-work (RTW) planning, and job accommodation. These interventions are geared toward helping the individual, but some may be designed to alter organizational behavior--offering improved depression screening and treatment training to primary care physicians and nurses, for example. Employer-level interventions are implemented by employers and focus on how the workplace itself can be constructed to promote mental health and prevent work disability. They typically involve modified work (such as offering employees with mental illnesses flexible work schedules), establishing a supportive work environment, or organization-wide mental health screening and training for human resources and supervisory staff to help them work with employees experiencing depression (Appendix A, Table A.4).
1. Individual-Level Studies
a. CMS' Demonstration to Maintain Independence and Employment (DMIE) did not improve the employment and earnings of workers with mental illness, but members of the intervention group were significantly less likely to receive Social Security disability benefits.
The DMIE was established to determine whether health-related EI strategies implemented by states could delay or prevent reliance on disability benefits and reduce job loss for working adults with disabilities. These RCT demonstrations enrolled adults aged 18-62 who worked at least part-time and were not receiving SSI or SSDI benefits. The DMIE was implemented in four states, which developed various service packages to provide medical benefits and financial assistance for health care (Whalen et al. 2012). Two states, Minnesota and Texas, focused on workers with behavioral health problems. We report on both the individual and pooled state results for these two states below.
In Minnesota, intervention participants (N=888) received such employment supports as care coordination, job placement, intensive employment-needs assessment, career counseling, worker support/coaching, Americans with Disabilities Act (ADA) disclosure training, and referrals to a workforce center. The control-group consisted of 267 individuals. With the exception of certain subgroups of participants, at one year follow-up, employment and earnings outcomes did not significantly differ between the intervention and control-groups; however, in contrast to similar participants in the intervention group, control-group members scoring below 50 on the Global Assessment of Functioning reported a decrease in income, suggesting that the intervention may have ameliorated a decline among low-functioning participants. Intervention group members who were more engaged with the program were significantly less likely to receive SSDI benefits than participants who were less engaged (Linkins et al. 2011).
Texas offered 888 randomly selected intervention participants enhanced mental health services and substance abuse assessment and referral services, dental and vision care, expedited clinic appointments, fully subsidized prescriptions and medical visits, durable medical equipment, podiatry, case management services, and transportation assistance at no cost. Another 697 individuals were randomly selected for the control-group. As in Minnesota, the evaluation found no significant differences in employment or earnings between the intervention and control-group members, but intervention participants were significantly less likely to receive SSI/SSDI (6 percent versus 8 percent) at follow-up (Bohman et al. 2011).
The pooled analysis of Minnesota and Texas intervention participants did not find an effect on the likelihood of employment but did show some evidence that the medical services DMIE provided decreased the adverse effect of mental illness on earnings for highly engaged, low-functioning individuals. Members of the intervention group were significantly less likely than those in the control-group to be receiving SSI disability benefits one year after DMIE enrollment (1.8 percent versus 3.2 percent), but no significant difference in annual earnings were found between the groups (Whalen et al. 2012). Because employment was examined for only one year after enrollment, long-term impacts are unknown.
b. Studies of individual-level clinical interventions for people with depression show limited evidence of improving employment outcomes.
Depression is the most studied mental illness with regard to the effect of interventions on employment outcomes. Nieuwenhuijsen et al. (2008) conducted a systematic review of interventions to improve occupational health in people with depression. The search returned 11 RCTs, all of which described worker-initiated, individual interventions. The only intervention found to have positive effects on sickness absence was psychodynamic therapy in combination with tricyclic antidepressant medication when compared to medication alone. The review did not find evidence of reduced sickness absence from the use of selective serotonin reuptake inhibitors, a computerized form of cognitive behavioral therapy, problem-solving therapy, enhanced primary care, or occupational therapy.
We identified two retrospective observational studies that used administrative data to examine the effects of antidepressant use on occupational outcomes. In the first study, Dewa et al. (2003) examined two years of administrative data on 1,281 employees from three large Canadian financial and insurance companies. They found that employees who went on long-term disability benefits were significantly less likely to fill any antidepressant prescriptions during a short-term episode. Moreover, EI (defined as guideline-recommended medication use within 30 days of short-term disability benefit start) was significantly associated with a reduced length of disability episode. In the second study, Burton et al. (2007) assembled a data set consisting of company personnel files, pharmacy claims records, and short-term disability claims for 2,112 employees at an American financial services company. Those who met antidepressant treatment adherence criteria during the three-month acute-phase follow-up period were significantly less likely to have any short-term disability absence. In the continuation-phase, adherent employees were less likely to have any short-term disability absence and less likely to have multiple short-term disability absences than non-adherent employees. Because those who were terminated during follow-up were excluded, the study does not provide information about the effect of adherence or short-term disability absences on job loss.
Adler et al. (2006) found that employees undergoing treatment for depression had worse job performance scores than healthy employees even after demonstrating clinical improvements in symptom severity. The study concluded that, although clinical interventions improve mental health, additional workplace interventions may be required to improve the performance of depressed employees.
2. Employer-Level Studies
a. There is limited evidence that interventions directed at the entire employee pool are effective for workers with mental illness.
Employer-level interventions often take the form of untargeted interventions, in which organizational changes are directed at the entire employee pool. These interventions typically focus on providing a supportive work environment, engaging in stress-reduction activities, and offering employees the opportunity to fully engage in the workplace (Lauber & Bowen 2010). Mental health education and awareness training programs are assumed to improve co-worker and supervisor support of colleagues with psychiatric disabilities (Krupa 2007), and there is evidence that strong supervisor and workplace social network supports produce positive effects on health outcomes and job performance (Lauber & Bowen 2010).
We identified one study with limited evidence of the effectiveness of interventions designed to increase awareness of mental health issues in the workplace. In a recent Finnish study (Vuori et al. 2012), an in-company training program was provided to employees of 17 medium-sized and large-sized organizations, with the goal of enhancing career-management, mental health, and job retention. Over the course of the study, 718 participants filled out a baseline questionnaire (which included questions on mental health status) and volunteered to participate in the program. Participants were randomized into intervention and comparison groups. The intervention group received a one-week group-training workshop focused on the enhancement of career-management skills. The comparison group received a literature package on basic career-management information. At the seven-month follow-up, the intervention group displayed significantly decreased depressive symptoms and intentions to retire compared with the comparison group. Although the study appears promising, its non-representative sample and lack of replication may limit its generalizability.
b. Although the extent to which employer provision of reasonable accommodations helps individuals remain employed is not well researched, accommodations may improve such employment outcomes as hours worked and job tenure and reduce job loss for individuals with psychiatric disabilities. However, disclosing one's disability during the process of requesting a reasonable accommodation bears some risk.
A literature review found 11 generally accepted categories of reasonable accommodations for people with psychiatric disabilities. But the benefits and risks inherent to employee disclosure of disability should be taken into account when evaluating the policy implications of employer-level interventions. The literature reveals little consensus on if, when, or how employees should disclose their disabilities to employers. The benefits of disclosure may include obtaining eligibility for protection against discrimination under the ADA, receiving support from such specialists as rehabilitation professionals, and the psychological benefits related to no longer hiding one's mental health conditions. Risks of disclosure include losing a promotion or a job, discrimination, and experiencing stigma at work (MacDonald-Wilson 2005).
Our literature review (O'Day et al. 2013) did not locate any high quality RCTs or well-controlled quasi-experimental studies measuring the employment outcomes of providing reasonable accommodations for individuals with psychiatric disabilities. To close this knowledge gap, Chow (2012) compared employment outcomes of participants in the EIDP who had received reasonable accommodations to those who had not. During the study period, participants who disclosed their mental health disability tended to receive a job accommodation and those with accommodations tended to work for longer periods of time; each accommodation decreased the risk of job loss by 12.7 percent. Participants with job accommodations worked an average of 7.68 hours more per month than those without accommodations at baseline. Average job tenure for individuals in the no-accommodations group was 157.47 days, whereas the accommodations group averaged 206.96 days. However, those who reported having an accommodation at work earned almost 5 percent less than those who reported having no accommodations. The author speculates that this finding might reflect wage discrimination faced by individuals who disclosed their condition to employers. Other unobservable factors related to employment might determine whether an employee discloses a disability and receives accommodation.4 There remains a substantial need for further research into the effects of reasonable accommodations on employment outcomes for individuals with mental health issues.
F. Evidence for Improving Employment Outcomes after a First Episode of Psychosis and for Transition-Age Youth
In this section, we discuss EI employment supports offered to individuals before or soon after a FE of psychosis and for TAY, which is commonly defined as ranging from 14-25 years old or 16-30 years old. The EI programs we reviewed are generally similar, with slight deviations along four dimensions: stage of illness, whether providers specialize in EI, the degree to which SE is integrated with mental health services, and the degree to which mental health services are comprehensive. The models tend to be adaptations of existing models used for populations with chronic mental illness, tailored to identify and appeal to people who are younger and whose conditions are not chronic. Functional and clinical recovery is the typical goal (Appendix A, Table A.5 and Table A.6).
EI models vary in the array of services offered and whether they are delivered by EI specialists. Most EI models offer multi-element services often through an interdisciplinary team. Many of the more comprehensive service models have modified the existing system of community mental health services (CMHS) for FE populations by forming interdisciplinary teams of EI specialists. Still other interventions are focused primarily on SE and do not include comprehensive, EI-specialist teams. Among the comprehensive models, services generally entailed a mix of medication management, cognitive therapy, social skills training, SE, and family intervention (family psychoeducation, for example) or family counseling. Some of the comprehensive, EI-specialist models have incorporated the IPS model as their vocational component. The psychosocial and vocational interventions are usually adapted to the age-specific needs of FE individuals by emphasizing education in addition to immediate job placement (Bird et al. 2010). Models commonly used for people with chronic SMI may be adapted in other ways as well; for example by emphasizing stress-reduction as a way of avoiding symptomatic and functional deterioration. Additionally, EI interventions are increasingly incorporating cognitive remediation (McFarlane et al. 2012).
1. Limited evidence suggests that individuals who experience a FE benefit more from comprehensive treatment services provided by EI specialists than from generic services designed for people with chronic mental illness.
Two studies compared comprehensive services provided by EI specialists and targeted to individuals experiencing FEs to generic (non-EI focused) services targeting the general population of mental health service users. Garety et al. (2006) randomized individuals in their 20s (with a mean age of 26) to comprehensive EI services provided by an EI team or generic services provided by a traditional mental health center without an integrated EI team and found that individuals who received EI services were significantly more likely to spend six months or more of the 18-month follow-up period engaged in work or education compared with controls (49 percent versus 24 percent). However, only one-third of the EI group was employed or enrolled in school full-time at follow-up and this rate was not significantly higher than that of the control-group. Fowler et al. (2009) compared participants in generic services provided by mental health centers (with teams of a psychiatrist and a case worker) to participants in "partial EI programs", which added EI specialists to the generic team from 1998 to 2002. In 2003, funds became available to implement a full service model, which added additional case managers and a vocational counselor to the team. Fowler added these participants to the study. Fowler found significant improvement among an EI group. One year post-referral, 40 percent of the EI cohort was competitively working or in school more than 15 hours per week during the assessment month, compared with significantly fewer (24 percent) of those who received "partial EI". Two years post-referral, 44 percent of the EI cohort were engaged in work or school more than 15 hours per week, significantly more than those in the "no-EI" group that received only generic services (15 percent).
2. Results suggest that individuals who receive comprehensive EI with integrated SE experience higher levels of employment.
Two small studies found promising results when they examined the issue of medical, vocational, and SE service integration. Researchers integrated an SE specialist or team into an existing EI service team. Existing EI services, which may or may not offer non-integrated vocational supports served as the comparison intervention. The interventions adapted SE for younger participants by providing supported education in addition to job placement.
Killackey et al. (2008) found that six months after enrollment, 13 out of 20 individuals experiencing FE randomized to comprehensive EI plus evidence-based SE found or retained employment, compared with two in the control-group. Major et al. (2010) found that at any time during the first 12 months of intervention, 36 percent of integrated EI treatment-group members gained or retained competitive employment and 20 percent began or remained in education, compared with 19 percent and 24 percent, respectively, in the standard EI group. Although these findings were significant, the sample sizes were quite small (20 and 44 respectively) and conclusions should be interpreted with caution.
3. One study suggests SE is also associated with positive outcomes when delivered outside of comprehensive EI services.
We identified one study that examined employment outcomes for individuals with FE or recent-onset psychosis receiving SE. This RCT differs from those discussed above in that SE was integrated into standard, generic CMHS. Those randomly assigned to the SE group additionally received a group-based work skills training, while the controls received referrals to VR, group-based communication skills, and medication management (Nuechterlein et al. 2008a). During the first six months of the program, significantly more individuals in the SE group had obtained or returned to employment or school than in the control-group (83 percent versus 41 percent). At the end of the 18-month intervention, by which time treatment intensity had faded, 72 percent of the SE group was employed or in education, compared to 42 percent of controls (Nuechterlein et al. 2008b).
4. Few studies reported the duration of employment or school enrollment. In those that did, participants were engaged in these activities only a small proportion of the time.
Of the nine studies reviewed, only two indicated the amount of time participants were engaged in work or school. In one of these, 49 percent of all EI individuals spent at least six months out of the 18-month study period employed or in an educational activity, which was significantly higher than the 29 percent among controls (Garety et al. 2006). In the other, those in the EI group who found employment worked, on average, significantly more weeks than those in the control-group: nine weeks compared to four weeks of the 26-week study period (Killackey et al. 2008). In this study, employment was substantial enough to significantly reduce reliance on Social Security disability or other cash benefits as a primary source of income (from 80 percent to 55 percent) but the majority of individuals remained on benefits (Killackey et al. 2008).5
5. Research on the effectiveness of SE for TAY is limited to one rigorous study, which showed promising results for young adults.
We identified two studies of SE with findings specific to TAY, but only one met our requirements for rigorous research (Burke-Miller et al. 2012). Results from that study were positive for older youth and mixed for younger ones. The authors analyzed subgroup results from EIDP to discern the effects of SE by age and determine how youth (ages 18-24) and young adults (ages 25-30) fared in comparison to adults ages 31 and older. They found that young adults in SE were significantly more likely to find competitive employment than were young adults who received services-as-usual or weaker forms of the intervention. In this study, about 70 percent of young adults found competitive employment, compared with about 40 percent who received services-as-usual or weaker versions of SE. Young adults in SE were also significantly more likely to find competitive employment than older adults in SE. Among youth ages 18-24, however, competitive employment rates did not significantly differ between those who received SE and those who received traditional services or weaker versions of SE, with about 45 percent of youth in both groups finding competitive employment.
6. More evidence is on the horizon.
We identified two new initiatives that will yield important evidence about the effectiveness of SE for people experiencing their FE of psychosis. Most notably, the National Institute of Mental Health is funding the Recovery after an Initial Schizophrenia Episode (RAISE) demonstration to test the clinical and cost-effectiveness of providing specialized FE care to individuals experiencing the early stages of schizophrenia. The RAISE demonstration consists of two complementary projects: an implementation study of delivering high quality FE care in clinics in New York and Maryland, and an RCT assessing the effect of providing an array of targeted services and supports early on to those with FE schizophrenia in 34 sites across the United States. The objective is to develop interventions that can be tested and readily adopted if they prove successful. The treatment models focus on intervening as soon as possible after the first symptoms or episode of schizophrenia and integrate medication, psychosocial therapies, family involvement, rehabilitation services, and SE. Results are expected in 2014.
The Early Detection, Intervention, and Prevention of Psychosis (EDIPP) Program, sponsored by the Robert Wood Johnson Foundation, expands a psychosis-prevention model to multiple sites around the country. EDIPP offers family-aided assertive community treatment (FACT) modified for EI to individuals at clinical high risk for psychosis. FACT includes psychoeducational multifamily group therapy, community-based treatment, SE and education, and psychotropic medication. Most of those in the comparison group, which consists of lower-risk youth, receive standard community clinical or psychosocial treatment, and some also receive supported education or employment (McFarlane et al. 2012). The results of EDIPP have not yet been published.
G. Other Services and Supports that Might Affect Employment Outcomes
In addition to the more rigorously evaluated types of employment supports described in preceding sections, a variety of other services have been postulated by stakeholders to positively affect employment outcomes. We reviewed information on several of these, including social enterprises, self-employment, consumer-provided services (which include peer counseling and other services provided by people with SMI or services provided by agencies staffed by people with SMI), self-determination models, asset-development, financial-literacy, and supported education (Appendix A, Table A.7). Although these interventions are considered promising, few high quality studies have been conducted to assess their effectiveness in comparison to alternatives. The interventions we reviewed have relatively small bases of rigorous evidence, or, in some cases, no rigorous evidence of their effectiveness. However, the evidence that does exist suggests that they can have positive effects on employment and mental health outcomes. More research is needed to establish the effectiveness of self-employment and consumer-run businesses, and on asset-development and financial-literacy programs. It is not immediately obvious how a rigorous study of self-employment could be conducted, although studies of supports for those who already are self-employed or are seeking self-employment would be feasible. Additional research on the efficacy of self-determination models for individuals with psychiatric disorders is needed; when these programs were first introduced, some were skeptical that individuals with SMI were well-suited to participate, so relatively little attention was paid to the outcomes of those who did.
The evidence for consumer-provided services is more substantial, but more work remains to be done to establish the most effective models for such programs. Consumer-provided services, defined as employment supports, peer counseling and other services provided by people with psychiatric disabilities or by agencies managed by people with psychiatric disabilities, are increasingly helping to fill in gaps and shortages in the mainstream mental health workforce, and a substantial percentage of consumer-operated service programs offer specific employment supports, such as resume preparation, job leads, and job seeker's support groups to help people find and retain jobs (Goldstrom et al. 2006). Moreover, these programs have the added advantage of providing direct employment to people with SMI.
The evidence for social enterprises is also growing. Social enterprises, also known as social firms, develop a business model with the goal of employing individuals from disadvantaged groups who would otherwise have a difficult time finding, obtaining, and maintaining a job. General guidelines for these enterprises call for at least 50 percent of revenue to come from sales, and at least 25 percent of employees to belong to a very disadvantaged group (McDermid et al. 2008). They may offer more flexible work conditions, provide targeted supports as an integrated part of the job, or simply encourage a more inclusive and supportive work atmosphere. Although any type of organization can use the social enterprise model, they tend to be established by non-profit organizations, or as free-standing non-profits. Results from one study suggest that social enterprises can increase job tenure, average weekly hours worked, quality of work life, and self-esteem among workers with psychiatric disorders (McKeown et al. 1992).
Evidence is beginning to emerge about the effectiveness of supported education. The evidence-based SE model has been adapted to include supported education; components generally include career planning, academic survival skills, help with enrollment and financial aid, and outreach to campus resource people.6 Research has shown that educational attainment is associated with the ability of people with psychiatric disabilities to obtain competitive employment (Burke et al. 2006), and the fastest-growing occupations are those requiring two-year or four-year college degrees or technical training (Cook & Burke 2002). Yet, few participants in SE programs have college degrees (Blyler 2003). In one study, the SE principle of rapid job search was modified to be a rapid enrollment in or return to relevant schooling for individuals who dropped out of school when they experienced a mental illness. The SE specialist assisted the participant to enroll or re-enroll in school programs consistent with their preferences and interests (Nuechterlein et al. 2008). Supported education appears to have substantial short-term benefits, some of which, like enrollment in education, suggest positive longer-term outcomes, but more research is needed to show that these long-term outcomes actually occur.
III. Evidence for Return-to-work and Employment-support Programs for Individuals with Other Disabilities
A. Introduction
In Chapter II, we reviewed evidence on the effectiveness of employment supports for individuals with SMI in the three target populations: individuals who are now or who are expected to be long-term clients of mental health agencies, employees at risk of job loss due to mental illness, and individuals experiencing a FE of psychosis and needing EI. ASPE is particularly interested in providing services and supports to enable people with SMI to find or keep employment, thereby reducing applications for Social Security disability benefits. In this chapter and the next one, we focus on individuals with other types of disabilities, and include information about the effectiveness of services to promote employment and the trajectory of service use prior to application for SSDI benefits. We summarize in this chapter an environmental scan we conducted to identify evidence of effectiveness of RTW or employment-support interventions for people with physical, developmental, or intellectual disabilities (Martin et al. 2013). The scan informed our discussion about effective services and supports for people with SMI (Appendix A, Table A.8).
RTW and employment-support interventions are intended to help people with disabilities and injured workers join or reintegrate into the workforce after a period of unemployment or sickness absence improve their health status and/or quality of life, and provide a cost-effective mechanism that will result in employment. RTW interventions are also intended to reduce the costs associated with loss of worker productivity and increased disability insurance benefits.
RTW interventions often extend beyond merely providing health care or medical services. For instance, they may include case management, workplace accommodations, integrated medical care and occupational training, or other strategies which vary in intensity or duration (van Oostrom et al. 2009). For those with early onset disabilities and limited or no work experience, employment supports often include habilitation services, which are intended to provide the necessary knowledge, skills, and abilities to obtain employment and reduce reliance on government-sponsored safety-net programs. For example, the state VR and the Ticket to Work (TTW) programs offer both rehabilitation and habilitation services.
In Section B, we describe disability management (DM) programs conducted by employers and the systematic reviews of these interventions. We included in our review interventions offered by health care providers if the intervention was initiated by the workplace or was integrated into the workplace. We included interventions with a primary goal of RTW; we did not include clinical studies that focused solely on health care or medical interventions. In Section C, we review demonstrations conducted by the Federal Government. In Section D and Section E, we review evidence of the effectiveness of VR and SE services, and in Section F, we review evidence of RTW programs conducted outside the United States.
B. Disability Management Programs
We identified several systematic reviews of DM or workplace disability management (WPDM) interventions. These DM interventions are primarily sponsored by employers and are aimed at employees with work limitations or endangered work tasks, or at individuals who have discontinued work. DM programs vary widely, depending on the employer and the impairment. There are no specific sets of services, and there is no specific model for DM or WPDM, which makes these programs difficult to evaluate through a systematic review. However, Gensby et al. (2012) list a range of components that can be included in DM or WPDM programs:
-
Early contact and intervention: communication and coordination of the RTW process between the employee and the employer.
-
Workplace assessment: a walk-through of the workplace to identify obstacles that might inhibit the absent employee from returning to work.
-
Provision of workplace accommodations: a reorganization of the job, or provision of equipment or other support that will enable the worker to return to the current job.
-
Transitional work opportunities: temporary tasks that can support the worker as he or she returns to full proficiency.
-
Modified and/or tailored work schedule or duties: special or light-duty jobs that enable an absent employee to return to work.
-
Access to alternative placements: assignment of the employee to another position to enable him/her to RTW.
-
RTW coordination or case management: a staff member who facilitates RTW services and functions, provides information, and coordinates services.
-
RTW policies: personnel and other policies that describe the procedures for dealing with sickness absence and the RTW process.
-
Active employee participation: involvement of the employee and co-workers in the RTW decision-making process.
-
Joint labor-management commitment: collaboration between management and employees regarding RTW.
-
Revision of workplace roles in RTW: re-defining tasks and delegating responsibilities to co-workers or supervisors while the employee is on leave.
-
Education of workplace staff: education and training for supervisors, union representatives, case managers, and others about RTW policies. These can be general education programs or they can be education on specific core components, such as how to discuss RTW components with employees, or coordination with medical staff.
-
Preventive strategies to avoid disability occurrence: reduction of workplace hazards that can contribute to disability.
-
Multidisciplinary work-rehabilitation services: vocational training, job replacement, job sharing, and job training; counseling, such as motivational or cognitive therapy; or other interventions, such as work adjustment or pain management.
Gensby et al. (2012) reviewed 13 DM studies published since 2010. Study participants included employees on sick leave who were unable to work due to disability.7 Most participants reported musculoskeletal disorders or low back pain (LBP). Although the 13 studies listed most of the DM components mentioned above, the authors could not determine whether specific DM program components or sets of components were driving effectiveness. They reported that the consistency and quality of the evidence is poor for WPDM interventions and concluded that there is a lack of evidence for determining the effectiveness of WPDM programs.
Another type of DM integrates WPDM with medical or health care interventions. We identified three systematic reviews of such interventions. Franche et al. (2005) conducted a systematic review of ten workplace-based interventions designed to assist workers--including those receiving workers' compensation--with musculoskeletal and other pain-related conditions. The interventions encompassed activities or supports in the workplace, as well as those outside of the workplace that used RTW coordinators as part of the workplace-based intervention. The authors reported strong evidence (based on findings from at least three studies of very high quality) that interventions that include an offer of a work accommodation, such as a change in job duties or work hours, or purchase of adaptive equipment, and early contact between the health care provider and the employer or workplace8 can reduce days on sick leave and workplace absence. The authors found moderate evidence that early employer contact with the absent worker,9 ergonomic visits to the worksite,10 and the presence of an RTW coordinator reduce workplace absence.
Williams et al. (2007) examined recently published research on the effectiveness of workplace-based rehabilitation interventions, including clinical interventions for workers with musculoskeletal work-related LBP. The authors synthesized 15 articles describing ten studies published since 2005 from the United States and other countries. The review included four RCTs and seven cohort studies with control-groups that were rated moderate to high in quality. The authors reported that workers who received the full treatment of clinical and workplace interventions, including fitness development, work hardening,11 and alternating days at the original job with increased tasks and days of functional therapy, as well as an ergonomic evaluation to determine the need for job modification, returned to work 2.4 times faster at statistically significant levels than workers who received usual clinical care. Workers who received early RTW/modified work interventions, defined as prompt assessment, rehabilitation, and treatment through modified work, also returned to work faster. Workers who received workplace site visits that were focused on ergonomic interventions reported a reduction in using sick leave, but the sample sizes were very small.
We found one systematic review of DM programs that occur outside the workplace. van Oostrom et al. (2009) examined the effectiveness of DM interventions at promoting "stay at work" through reducing sickness absence among people with musculoskeletal conditions, mental health problems, and other health conditions. The authors conducted a meta-analysis of six RCTs--from the United States and other countries--that considered several impairment types: LBP, upper extremity disorders, and musculoskeletal impairments. They compared DM interventions, including changes to the workplace or equipment (such as alterations to the furniture or equipment needed to do the job), work design and organization (including changes in duties or tasks), working conditions or environment (such as lighting or noise), and case management with active involvement of the worker and employer (meaning at least one face-to-face discussion between the worker and the employer) to usual care. The authors found five RCT studies on employees with musculoskeletal disorders and one on individuals with mental health disorders. The authors concluded that there was moderate evidence of the effectiveness of workplace interventions to reduce employee absence compared to usual care for musculoskeletal disorders but little evidence for other groups due to the lack of RCT studies.
C. Demonstrations by the Social Security Administration to Improve Return-to-Work and Reduce Participation in Disability Programs
There is considerable policy concern about and interest in interventions designed to help SSI and SSDI beneficiaries find or resume work. We identified two rigorous evaluations of interventions targeted to SSI or SSDI beneficiaries that have been conducted in the last ten years. The quasi-experimental evaluation of SSA's TTW program assessed the impact of the program on service enrollment and employment. TTW allows beneficiaries to deposit a "Ticket" with one of a range of public or private employment service providers, including state VR agencies. The program expanded beneficiary choice of SSA-sponsored service providers over the traditional system, in which SSA reimbursed only state VR agencies for serving beneficiaries. Initial findings of the TTW evaluation did not show significant impacts of the program on beneficiary employment, but later findings showed that TTW and related programs are having a limited but positive effect on employment for SSI and SSDI beneficiaries, and have motivated some beneficiaries to pursue employment (Livermore et al. 2013). Although relatively few beneficiaries continue to be enrolled in TTW, those who use TTW and other programs have better employment outcomes than those who do not.
Fraker et al. (2013) are currently conducting an evaluation of the Youth Transition Demonstration (YTD), a rigorous experimental evaluation of six employment-support projects designed to identify interventions that will improve the educational and vocational outcomes for youth (ages 14-25). Approximately 880 youths at each site who agreed to participate in the evaluation were randomly assigned to treatment or control-groups. Each of the YTD sites offered individualized work-based experiences, including internships, job shadowing, job coaching, and competitive paid employment; waivers of various SSI rules to promote employment; and benefits counseling to teach youths about these work incentives. The sites also offered empowerment training to help participating youth learn to make their own choices (as opposed to having a parent or guardian direct those choices). The control-group received standard disability program work incentives and whatever alternative services were available in their communities.
The YTD evaluation is tracking employment, earnings, and receipt of disability benefits. Preliminary results one year after study enrollment vary by site. Three of the six sites had a significant positive impact--of between 9 and 19 percentage points--on whether the youth had held a job. One of these sites also showed significant impacts on total earnings (a difference of $524 and $306 in annual earnings) (Fraker et al. 2011). The other three sites showed no significant impacts one year after enrollment.
D. State Vocational Rehabilitation Programs
In the United States, VR refers to training and supports for persons to obtain work, return to work, or stay at work. There are different types of rehabilitation programs (for example, medical and vocational) and various organizations and funding sources that support rehabilitation services, including federal, state, and private entities. Although the organizations and funding sources for rehabilitation can overlap, the central focus of this section is on VR interventions offered through financing mechanisms of the U.S. Department of Education's Rehabilitation Services Administration (RSA). The RSA-sponsored state-federal program is by far the largest VR program offering employment-support interventions to help individuals with disabilities obtain employment. Title I of the Rehabilitation Act of 1973 authorizes a VR program to provide services to persons with disabilities so they can prepare for and engage in gainful employment. Each state and territory designates a single VR agency to administer the VR program, except where state law authorizes a separate agency to administer VR services for blind individuals.
VR counselors are professionals who work with individuals with disabilities to develop a rehabilitation plan for employment. VR interventions are tailored for each client, and may include a broad array of services, such as counseling; assistive technology; vocational training; or funding for higher education, job search, or job-placement assistance and SE.12
Numerous studies have been conducted on the federal-state VR program, and most indicate that intensive job readiness, job placement, and SE are associated with competitive employment outcomes at a statistically significant level (Pruett et al. 2008; Ownsworth & McKenna 2004; Saunders et al. 2006). However, many VR studies do not sufficiently control for outside factors, and there is seldom a satisfactory control-group, making it difficult to determine the relative employment outcomes for people with disabilities in the absence of VR services (Livermore & Goodman 2009).
E. Supported Employment
SE can be described as a form of competitive employment in which rapid job search and placement is followed by intensive on-the-job support provided to an individual with a disability for a certain period, followed by extended services to support job maintenance. It is distinguished from SE for people with mental health disabilities (described in Chapter II) because: (a) it does not necessarily integrate mental health service providers into the support team; and (b) a specific model of SE has not been rigorously tested with people with other disabilities. SE is distinguished from DM in part through the populations served: people with severe intellectual and other developmental disabilities, SMI, or others with limited or no work record, versus workers who acquire a disability, have a work record, and wish to continue working. Another distinguishing factor is the strong evidence base for a specific SE model for people with SMI, versus lack of evidence and a universally accepted model for DM. A third factor is that SE typically does not include a medical component, although SE for people with SMI does include a mental health professional on the team.
We identified two systematic reviews of SE or VR interventions for young adults with Autism Spectrum Disorder (ASD) (Lounds-Taylor et al. 2012; Westbrook et al. 2012.). The authors of these studies summarized findings from five studies on young adults (ages 13-30) with ASD and other developmental disabilities. Overall, both sets of authors reported that on-the-job supports were associated with increased employment outcomes for persons with ASD and other developmental disabilities, but evidence was limited for on-the-job supports for individuals with ASD. Thus, the results do not support reliable conclusions about the effectiveness of employment services for adults with ASD.
F. Reviewed of Employment Interventions Outside the United States
We explored systematic reviews of RTW interventions in Organisation for Economic Co-operation and Development (OECD) countries, such as the United Kingdom, Canada, Finland, Sweden, the Netherlands, and others. Carroll et al. (2010) conducted a systematic review comparing workplace and non-workplace interventions for persons with back pain. He found ten articles reporting nine trials from Europe and Canada, and four articles evaluating the cost-effectiveness of interventions. The majority of the trials were of good or moderate quality. Participants in eight trials had back pain and related musculoskeletal conditions, and consisted of full-time or part-time employees on long-term sick leave at the time of the intervention. The authors reported that interventions involving employees, health practitioners, and employers working together to implement work modifications were more consistently effective than those that do not possess such components. The authors also found EI to be effective. Economic evaluations indicated that interventions with a workplace component are likely to be more cost-effective than those without. The authors concluded that stakeholder participation and work modification were more effective and cost-effective than other workplace-linked interventions, including exercise, at returning adults with musculoskeletal conditions to work.
Schandelmaier et al. (2012) conducted a systematic review of the effectiveness of interventions involving RTW coordination compared to usual practice in patients at risk for long-term disabilities, focusing on private disability insurance or third-party RTW providers. The authors conducted a meta-analysis of nine trials from OECD countries, including one from the United States. Employers provided the interventions and included employees who had been absent from work for at least four weeks. The majority of participants reported musculoskeletal disorders and LBP. Overall, the authors found moderate evidence that RTW coordination interventions resulted in small relative increases in RTW but found no evidence that one type of RTW coordination program was superior to another.
Dibben et al. (2012) conducted a systematic review of RTW studies published between 2005 and 2011. The review focused primarily on evidence from the United Kingdom, but included findings from the United States and other countries. Interventions were designed to help people with common health conditions stay at or return to work, and included workplace-based cognitive behavioral therapy, workplace-based patient education, VR, and encouragement of physical activity. The authors reported a strong body of evidence, with positive effects, for workplace-based interventions for those with musculoskeletal disorders (particularly LBP), including cognitive behavioral therapy, VR, and workplace rehabilitation. Similar to Schandelmaier et al. (2012), the authors reported some evidence of the benefits gained from coordination with rehabilitation professionals. Dibben et al. noted that evidence of effectiveness for other interventions was based on an insufficient number of studies, studies of poor quality, or studies that were inconclusive. The authors suggested there is a need to consider longer-term outcomes to assess sustainability of DM interventions.
IV. Pre-application Work Activity of Social Security Disability Insurance Applicants
A. Introduction
In this chapter, we describe the employment and program-participation patterns of people with disabilities before they applied for SSDI. ASPE is interested in understanding these characteristics so it can recommend policies and programs to help potential applicants remain in the workforce, thereby stemming the growth in the SSDI rolls. To uncover these patterns, we used SIPP data matched to SSA administrative data to compile statistics on several characteristics of SSDI applicants and to answer the following two questions:
-
What are the demographic, employment, and program-participation characteristics of SSDI applicants before they apply for SSDI?
-
What are the demographic, employment, and program-participation characteristics of at-risk group members who later apply for SSDI?13
Although relatively few studies have uncovered the employment and program-participation paths of eventual SSDI applicants and recipients, a few things are known. The lives of SSDI applicants before application are often characterized by a disruptive change in health, separation from employment, and a period of time between job separation and applying for SSDI (Lindner 2013). Most SSDI applicants stop work for health-related reasons, such as the onset of a work limitation, rather than because of layoff or resignation. Those who leave because of illness or injury are more likely to apply for SSDI quickly, and they are less likely to seek other work. Individuals who receive SSDI are less likely than those who do not to have health coverage for as many as three years before they receive benefits (Livermore et al. 2010). SSDI applicants are also influenced by the current business cycle (Coe & Rutledge 2013). During a recession, individuals may perceive their employment to be more unstable and replacement work more difficult to find, increasing the likelihood they will apply for SSDI.
Using the Panel Study of Income Dynamics from 1970 through 1991, Daly (1998) found that 25 percent of SSDI beneficiaries received some type of public assistance in the five years before receiving SSDI benefits and 83 percent received some type of public transfer benefit. Honeycutt (2004), using the Current Population Survey and the SIPP, found that individuals enrolled in employer disability benefits, other types of disability income, or Medicaid were the most likely to later access SSDI; those who received workers' compensation, food stamps, utility assistance, or retirement income, or those who lacked health insurance coverage had a moderate likelihood of later receiving SSDI. Analysis by Lindner & Nichols (2012) revealed that improved access to unemployment insurance benefits reduced SSDI applications, at least in the short term.
| TABLE IV.1. Definition of At-Risk Groups | |
|---|---|
| At-Risk Group | Definition |
| Unemployment benefit recipients | Individuals with a work limitation who began receiving unemployment benefits after the first interview wave. |
| Workers at risk of unemployment benefit receipt | Individuals with a disability who worked in the first interview wave and who scored in the top 33% based on a model predicting unemployment benefit receipt within 36 months. |
| Individuals with high health expenditures | Individuals who had out-of-pocket health expenditures, not including health insurance premiums, in the past year that equaled or exceeded 7.5% of their household income. This mirrors federal tax law, which allowed individuals to claim out-of-pocket health expenses above 7.5% as a tax deduction. (In 2013, this percentage increased to 10%.) Health expenditures are available only in topical modules 3 and 6. |
| Workers' compensation beneficiaries | Individuals who began receiving workers' compensation benefits after the first interview wave. |
| Private disability beneficiaries | Individuals who began receiving employer or individual disability benefits after the first interview wave. |
| Veterans with disabilities | Individuals with a disability who reported being a veteran in the first interview wave. |
| Recipients of job training or education services | Individuals with a work limitation who reported in wave 2 participating in job training or education services in the past 12 months. |
For this analysis, we use SIPP data matched to SSA administrative records to examine the characteristics of all individuals who applied to SSDI within six years of their first SIPP interview.14 We further explore the characteristics of individuals within seven groups who are at risk of applying for and receiving SSDI. The at-risk groups include: unemployment insurance recipients with a disability, workers with disabilities who are at risk of applying for unemployment insurance benefits, individuals with high health expenditures, workers' compensation beneficiaries, private disability insurance beneficiaries, military veterans with a disability, and individuals with disabilities who received job training or education services within the past year (Table IV.1). The disability definition used for the above categories is the work limitation question from the first SIPP wave. The individuals in these groups might overlap (that is, an individual in the veterans group could also be an individual with high health expenditures). We examined various characteristics--including demographic variables (age, gender, race, marital status, and educational attainment) as well as specific employment, income and program-participation measures (defined in Table IV.2)--for each group. We restrict the sample to individuals 25-55 years old because individuals younger than that are less likely to qualify for SSDI and individuals older than that can qualify for Social Security early retirement benefits during our six-year observation period. We provide a fuller description of our methods in Appendix C. The results presented here come from a working paper, conducted through SSA's Disability Research Center, on the experiences of SSDI applicants before they apply for benefits (Thompkins et al. forthcoming).
| TABLE IV.2. Definitions of Employment, Income, and Program Participation | |
|---|---|
| Measure | Definition |
| Employment and Income | |
| Any employment | Reported having a job for any month during the specified period. |
| Without a job and not looking for work | Reported not having a job and not looking for work for any month during the specified period. |
| Individual earned income | The individual's average monthly earned income during the specified period. |
| Individual total income | The individual's average monthly earned and unearned income during the specified period. |
| Household total income | The household's average monthly earned and unearned income. |
| Households under FPL | A comparison of the household's total income relative to 100% of FPL. |
| Program Participation | |
| SNAP | Household receipt of food stamps. |
| Energy assistance | Household receipt of federal, state, or local energy assistance. |
| Subsidized housing | Household receipt of housing assistance or subsidized rental assistance. |
| TANF | Household receipt of TANF (or, for the first 3 waves of the 1996 SIPP panel, Aid to Families with Dependent Children). |
| SSI | Receipt of SSI benefits due to disability (from SSA administrative data). |
| Employer-based disability insurance | Receipt of disability insurance benefits through one's employer. |
| Own sickness or disability insurance | Receipt of benefits through a personal sickness, accident, or disability policy. |
| Workers' compensation | Receipt of workers' compensation income in one's own name. |
| Medicaid | Receipt of Medicaid health coverage in one's own name. |
| Private health insurance | Covered by health insurance other than Medicaid and Medicare. |
| Unemployment benefits | Receipt of state unemployment compensation benefits in one's own name. |
| Veterans' benefits | Receipt of veterans' benefits in one's own name. |
B. Results
1. Demographic characteristics of SSDI applicants and at-risk group members.
The demographic characteristics of SSDI applicants in our sample are similar to those in previous studies. Compared to all individuals ages 25-55, SSDI applicants were significantly more likely to be older, Black, divorced, have less education, and have lower household incomes (Table IV.3). Members of the high-risk groups we examined had similar demographic characteristics as SSDI applicants, though many groups had higher proportions of individuals who were younger, who were White, and who had more education compared to SSDI applicants.
| TABLE IV.3. Demographic Characteristics of SSDI Applicants and At-Risk Group Members | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| SSDI Applicants | Unemployment Insurance | Workers At Risk of Unemployment Insurance | High Health Expenditures | Workers' Compensation | Private Disability Insurance | Veteran's | Job Training/ Education Services | All Individuals Ages 25-55 | |
| Female | 53.0% | 45.0% | 50.4% | 56.6% | 46.1% | 51.8% | 9.7%** | 54.2% | 50.9% |
| Age (mean) | 44.7 | 42.3* | 41.1* | 41.7* | 41.9* | 44.2 | 45.7 | 42.2* | 39.4** |
| Race | |||||||||
| Asian | 1.6% | 1.6% | 0.9% | 2.8% | 2.9% | 2.6% | 0.7% | 1.0% | 4.2%** |
| Black | 19.4% | 13.4% | 10.2%* | 10.1%* | 15.2% | 16.3% | 17.3% | 11.8%* | 11.9%** |
| White | 76.1% | 82.2% | 87.0%* | 85.5%* | 79.4% | 78.5% | 78.3% | 84.7%* | 82.1%** |
| Other | 2.9% | 2.8% | 2.0% | 1.7% | 2.6% | 2.7% | 3.7% | 2.5% | 1.8% |
| Marital Status | |||||||||
| Married | 53.4% | 52.2% | 35.2%* | 49.7% | 56.3% | 54.8% | 55.8% | 56.1% | 64.5%** |
| Never married | 18.2% | 20.5% | 32.1%* | 20.9% | 19.7% | 20.1% | 13.9% | 20.4% | 19.1% |
| Widowed | 2.5% | 2.2% | 2.7% | 2.8% | 2.0% | 2.7% | 1.3% | 1.9% | 1.2% |
| Divorced | 20.9% | 20.9% | 23.9% | 22.3% | 17.4% | 17.6% | 24.3% | 17.7% | 12.2%** |
| Separated | 5.1% | 4.3% | 6.2% | 4.2% | 4.5% | 4.8% | 4.7% | 3.8% | 3.0%* |
| Educational Attainment | |||||||||
| Less than high school diploma | 20.0% | 17.9% | 25.3% | 11.8%* | 18.0% | 15.4% | 8.3%* | 7.7%* | 11.8%** |
| High school diploma/GED | 34.4% | 32.5% | 46.0%* | 29.9% | 37.9% | 32.1% | 34.1% | 23.2%* | 28.2%** |
| Some college | 36.0% | 39.1% | 22.1%* | 34.6% | 32.1% | 37.1% | 45.9%* | 44.7%* | 32.1% |
| Four-year college degree or more | 9.7% | 10.4% | 6.6% | 23.7% | 12.0% | 15.4% | 11.7% | 24.4%* | 27.8%** |
| Monthly Household Income | $2,802 | $3,820* | $3,625* | $3,240* | $5,402* | $5,428* | $3,931* | $5,146* | $5,783** |
| Applied to SSDI | |||||||||
| Number | 3,380,365 | 68,849 | 99,095 | 251,233 | 161,671 | 176,550 | 153,821 | 114,687 | 3,380,365 |
| Percent | 100.0% | 13.3% | 14.7% | 5.6% | 13.9% | 21.7% | 12.7% | 9.0% | 2.8% |
| Unweighted Sample Size | 3,754 | 559 | 714 | 4,768 | 1,234 | 860 | 1,285 | 1,365 | 127,972 |
| Weighted Sample Size (average per panel) | 3,380,365 | 516,976 | 674,944 | 4,491,099 | 1,162,518 | 813,566 | 1,208,894 | 1,268,832 | 121,410,365 |
| SOURCE: 1996, 2001, and 2004 SIPP panels. NOTES: Demographic characteristics of SSDI applicants and of at-risk group members at the time they were identified as group members are shown in the table. The statistics for "individuals ages 25-55" are for individuals ages 25-55 in wave 1 of each panel, regardless of disability, SSDI, or at-risk group status. Statistics for SSDI applicants were compared to individuals ages 25-55; statistics for at-risk groups were compared to SSDI applicants. T-tests used for all statistical comparisons. * p<0.05 ** p<0.01 | |||||||||
Among the at-risk groups (Table IV.3), the private disability insurance group had the highest proportion of individuals who turned to SSDI for support. More than one-fifth (22 percent) of those receiving private disability insurance applied to SSDI during the observation period. Workers with disabilities who were at risk of obtaining unemployment insurance benefits (15 percent), workers compensation beneficiaries (14 percent), and those who received unemployment insurance benefits (13 percent) had the next-highest proportions of SSDI applicants. Individuals with high health expenditures had the lowest rates of SSDI application across our at-risk groups; 6 percent of such individuals eventually applied for benefits. This proportion, however, is twice that which is observed in the general population of adults who are ages 25-55 (3 percent of whomapplied for SSDI benefits).
Even though a group had a high proportion of individuals who applied for SSDI, the relative number of them compared to all SSDI applicants might be small. For instance, although 22 percent of individuals with private disability insurance benefits applied to SSDI, no more than 8 percent of SSDI applicants (as will be seen in the next section) had such benefits (either employer-based disability or one's own sickness or accident insurance) at the time of their application.
2. Experiences of SSDI applicants before application.
SSDI applicants experienced a consistent decline in employment and income--and an increase in the likelihood of being out of the labor market entirely--as early as more than two years before SSDI application. In Figure IV.1, we show two statistics: (1) the proportion of SSDI applicants who were employed; and (2) the proportion who were without a job and not looking for work. Both statistics are calculated when reported for at least one month in the six-month intervals before SSDI application, and so are not mutually exclusive; data are shown in Appendix D, Table D.1. From 37 months to 42 months before they applied, 89 percent of applicants worked (compared to 84 percent of the general population ages 25-55 in the first SIPP wave), and 18 percent were without a job and not looking for work at any point during the six-month period (compared to 17 percent of the general population). As individuals approached SSDI application, the proportion employed declined substantially--to 66 percent in the six-month period before SSDI application--and more than half of applicants (54 percent) had at least one month in which they were neither working nor looking for a job. This pattern shows that, for many SSDI applicants, the attachment to the labor market was strong up to three years before SSDI application. In Appendix D, Table D.1, we include three measures of mean income of SSDI applicants at six-month intervals before benefit application, as well as a measure of poverty (the proportion with household incomes below the FPL). At 37-42 months before SSDI application, the mean monthly individual earned income, earned income of those with earnings, individual total income, and household total income of SSDI applicants were $1,887, $2,364, $2,068, and $3,923, respectively; 24 percent of SSDI applicants were below FPL. (The respective numbers for the general working-age population were $2,727, $3,399, $2,892, and $5,783, and 13.4 percent). In the six months before SSDI application, the mean individual monthly earned income of SSDI applicants fell to $944 (though of those with earnings, this value declined only to $1,941), the mean monthly household total income fell to $3,359, and the proportion living below FPL increased to 40 percent. These patterns are consistent with the previously noted decreasing labor-market connection among SSDI applicants. Additionally, mean individual income fell by less than the mean individual earned income of SSDI applicants. This suggests that future SSDI applicants partially offset their declining earnings by making use of programs that provide financial-support.
| FIGURE IV.1. Labor Force Participation of SSDI Applicants |
|---|
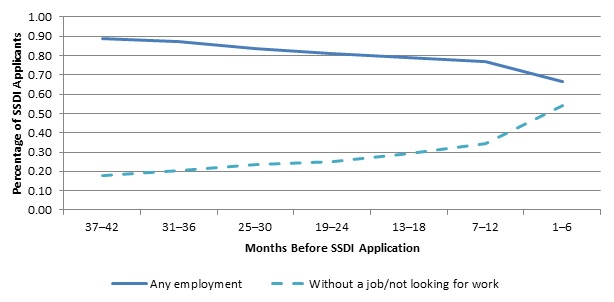 |
When we examine program participation before SSDI application, we discover a larger proportion of SSDI applicants who received means-tested benefits up to 36 months before applying for SSDI, compared to the individuals ages 25-55 (Table IV.4). Between 10 percent and 21 percent of eventual SSDI applicants received benefits from Supplemental Nutrition Assistance Program (SNAP) during the 42 months before SSDI application, 4-8 percent received energy assistance, and 2-3 percent received housing assistance. Benefit receipt tended to increase in the six-month period before SSDI application, and the proportion of SSDI applicants receiving such benefits was typically greater than for the working-age population across the 42-month period before SSDI application. Among disability-related benefits, the proportion of SSDI applicants who received SSI was less than 1 percent and no different than for the working-age population. A relatively small proportion of SSDI applicants was involved in other programs related to disability or health (their own or employer-based disability coverage or workers' compensation) in the 42-month period leading up to SSDI application, though--as with poverty-related benefits--the proportion tended to increase in the six months just before application. Regarding health insurance coverage, a majority of individuals (from 67 percent to 73 percent) had private health insurance before SSDI application, even in the period just before SSDI application, although that percentage declined as individuals approached SSDI application. Between 11 percent and 20 percent of applicants reported having Medicaid coverage. Relatively few individuals who entered the SSDI program received unemployment or veterans' benefits up to 42 months before SSDI application; participation in these programs was stable across the observed periods.
| TABLE IV.4. Program Participation of SSDI Applicants | ||||||||
|---|---|---|---|---|---|---|---|---|
| 37-42 Months Before SSDI Application | 31-36 Months Before SSDI Application | 25-30 Months Before SSDI Application | 19-24 Months Before SSDI Application | 13-18 Months Before SSDI Application | 7-12 Months Before SSDI Application | 1-6 Months Before SSDI Application | All Individuals Ages 25-55 | |
| Poverty-Related Benefits | ||||||||
| SNAP | 10.2%* | 12.6%* | 10.7%** | 12.4%* | 13.2%* | 15.2% | 21.1% | 4.0%** |
| Energy assistance | 4.1% | 5.6% | 5.1% | 5.7% | 5.2% | 5.4% | 7.6% | 2.1%** |
| Subsidized housing | 2.8% | 3.4% | 2.7% | 2.3% | 1.7% | 2.2% | 2.8% | 1.2% |
| TANF | 3.7% | 2.9% | 2.6% | 2.2% | 2.9% | 3.6% | 4.7% | 1.2%* |
| Disability-Related Benefits | ||||||||
| SSI | 0.5% | 0.3% | 0.5% | 0.5% | 0.7% | 0.9% | 1.0% | 1.1% |
| Employer-based disability insurance | 0.0%** | 0.0%** | 0.7%** | 0.8%** | 1.1%** | 2.7% | 6.5% | 0.2%** |
| Own sickness or accident insurance | 0.0%* | 0.3% | 0.2%* | 0.4% | 0.4% | 1.2% | 2.1% | 0.0%* |
| Workers' compensation | 4.1% | 3.9%* | 1.7%** | 2.6%** | 4.4%* | 5.6% | 9.3% | 0.4%** |
| Health Insurance | ||||||||
| Medicaid | 10.6%* | 11.9%* | 12.1%* | 11.8%* | 13.8% | 15.9% | 20.4% | 6.1%** |
| Private health insurance | 72.9% | 72.0% | 70.3% | 71.1% | 67.5% | 67.4% | 66.7% | 77.9%** |
| Employment-Related Benefits | ||||||||
| Unemployment benefits | 7.5% | 5.7% | 6.4% | 7.2% | 5.4% | 5.9% | 7.5% | 2.4%** |
| Veterans' benefits | 1.7% | 1.9% | 3.4% | 3.6% | 3.7% | 3.3% | 3.2% | 0.7%* |
| Unweighted Sample Size | 204 | 376 | 626 | 856 | 1,045 | 1,202 | 1,335 | 127,972 |
| Weighted Sample Size (average per panel) | 173,487 | 322,895 | 556,766 | 762,919 | 939,560 | 1,094,278 | 1,219,322 | 121,410,365 |
| SOURCE: 1996, 2001, and 2004 SIPP panels matched to SSA administrative data. NOTES: Participation of SSDI applicants in 6-month intervals before they applied for benefits is shown in the table. The statistics for "individuals ages 25-55" are for individuals ages 25-55 in wave 1 of each panel, regardless of disability, SSDI Application, or at-risk group status. The table includes 2 types of comparisons using t-test statistics: (1) each 6-month period was compared to 1-6 Months Before SSDI Application; and (2) the period of 1-6 Months Before SSDI Application was compared to individuals ages 25-55. * p<0.05 ** p<0.01 | ||||||||
3. Experiences of individuals in the at-risk groups.
Six of the seven at-risk groups had sufficient sample sizes of SSDI applicants to make comparisons; individuals with unemployment benefits were excluded from the analyses. Although at-risk group members who eventually applied for SSDI tended to have lower rates of employment (and higher rates of being out of the labor market), the differences tended not to be statistically significant, though the patterns across at-risk groups were often similar (Table IV.5). Individuals in the high health expenditure, training, veterans with disabilities, and workers' compensation groups who eventually applied for SSDI had similar employment rates during the earliest six months of the observation period (that is, directly after being identified in the at-risk group). Alternatively, individuals receiving private disability insurance who applied for SSDI at first had employment rates that were larger than those who did not apply; the proportions reversed, however, by the 13-18 month observation period. No matter the starting point, the differences in employment rates for all groups between eventual SSDI applicants and non-applicants increased over time. For instance, the difference in the employment rates for veterans with disabilities who did and did not apply was 6 percentage points in the first six-month period; that difference increased to 16 percentage points by 31-36 months. This pattern is because the employment rates of those who did not apply to SSDI remained fairly constant while the employment rates of those who did apply to SSDI declined.
In Table IV.6, we show the relative timing of SSDI application for individuals in each at-risk group. About half or more of individuals who received private disability insurance or workers' compensation benefits applied to SSDI within the first six months of receiving the benefit, whereas individuals in the other at-risk groups were more evenly distributed across the six-year period for which we observed SSDI applications. Because we examined SSDI application in a six-year period from the date of the first SIPP interview, data for most groups are right censored; individuals could have been identified as being in an at-risk group after the beginning of the first SIPP wave (for instance, those whose first receipt of private disability insurance occurred in year 2 of the SIPP) and therefore did not have a full six years of observation.
| TABLE IV.5. Employment of SSDI Applicants and Non-Applicants, by At-Risk Group | ||||||
|---|---|---|---|---|---|---|
| At-Risk Group | 1-6 Months | 7-12 Months | 13-18 Months | 19-24 Months | 25-30 Months | 31-36 Months |
| Eventually Applied for SSDI Benefits | ||||||
| High health expenditures | 77.0% | 71.1% | 61.8%* | 54.5%** | 58.2%* | 55.8%* |
| Private disability insurance | 72.4% | 54.6% | 41.7% | ND | ND | ND |
| Job training | 83.8% | 78.1% | 74.3% | 69.4% | 62.5% | 61.3% |
| At risk of unemployment insurance | 100.0% | 91.6% | 81.9% | 78.8% | 74.1% | ND |
| Veterans | 58.3% | 55.1% | 50.2% | 52.5% | 44.8% | 55.0% |
| Workers' compensation | 59.9% | 51.8% | 44.8% | 46.3% | ND | ND |
| Did Not Apply for SSDI Benefits | ||||||
| High health expenditures | 81.2% | 82.4% | 81.1% | 82.4% | 82.1% | 82.3% |
| Private disability insurance | 62.4% | 61.7% | 63.2% | 64.4% | 63.9% | 68.4% |
| Job training | 89.4% | 89.2% | 89.1% | 87.5% | 88.9% | 87.2% |
| At risk of unemployment insurance | 100.0% | 95.3% | 90.4% | 91.5% | 87.9% | 87.3% |
| Veterans | 64.6% | 66.1% | 66.0% | 67.6% | 66.4% | 70.8% |
| Workers' compensation | 63.3% | 64.1% | 64.9% | 68.3% | 67.5% | 63.8% |
| SOURCE: 1996, 2001, and 2004 SIPP panels matched to SSA administrative data. NOTES: Employment characteristics of at-risk group members in 6-month intervals after they were identified in the at-risk group are shown in the table. Sample sizes are in Appendix Table D.2. ND = no data (sample size fewer than 50). * p<0.05 ** p<0.01 | ||||||
| TABLE IV.6. Timing of SSDI Application for All SSDI Applicants and At-Risk Groups of SSDI Applicants | |||||||
|---|---|---|---|---|---|---|---|
| Group | N | Year 1 | Year 2 | Year 3 | Year 4 | Year 5 | Year 6 |
| All SSDI applicants | 3,754 | 16% | 17% | 16% | 16% | 16% | 19% |
| High health expenditures | 275 | 25% | 19% | 18% | 16% | 22% | 0% |
| Private disability insurance | 186 | 66% | 15% | 6% | 9% | 4% | 0% |
| Job training | 125 | 23% | 12% | 21% | 18% | 16% | 9% |
| Unemployment insurance | 78 | 38% | 17% | 19% | 13% | 14% | a |
| At risk of unemployment insurance | 108 | 23% | 13% | 17% | 13% | 18% | 16% |
| Veterans | 166 | 26% | 18% | 19% | 11% | 13% | 13% |
| Workers' compensation | 172 | 50% | 22% | 17% | 11% | a | a |
| SOURCE: 1996, 2001, and 2004 SIPP panels matched to SSA administrative data. NOTES: Table shows the year, relative to being identified as a group member, in which individuals applied to SSDI. For SSDI applicants, the year is relative to the SIPP start date.
| |||||||
| TABLE IV.7. Selected Program Participation and Incomes of SSDI Applicants and Non-Applicants, by At-Risk Group | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Program or Income Variable/ Period | High Health Expenditures | Private Disability Insurance | Job Training | Workers At Risk of Unemployment Insurance | Veterans | Workers' Compensation | ||||||
| SSDI Applicants | Non- Applicants | SSDI Applicants | Non- Applicants | SSDI Applicants | Non- Applicants | SSDI Applicants | Non- Applicants | SSDI Applicants | Non- Applicants | SSDI Applicants | Non- Applicants | |
| Sample Size | ||||||||||||
| 1-6 months | 243 | 3,882 | 144 | 518 | 112 | 1,091 | 108 | 602 | 158 | 942 | 139 | 863 |
| 7-12 months | 226 | 3,717 | 107 | 355 | 108 | 1,043 | 105 | 592 | 141 | 816 | 110 | 597 |
| 13-18 months | 177 | 2,945 | 87 | 287 | 105 | 974 | 106 | 593 | 136 | 793 | 96 | 503 |
| 19-24 months | 132 | 2,429 | ND | 167 | 79 | 783 | 105 | 589 | 118 | 697 | 52 | 301 |
| 25-30 months | 100 | 1,512 | ND | 105 | 50 | 465 | 80 | 457 | 103 | 582 | ND | 238 |
| 31-36 months | 98 | 1,482 | ND | 52 | 52 | 459 | ND | 232 | 55 | 187 | ND | 136 |
| SNAP | ||||||||||||
| 1-6 months | 15.7% | 5.1% | 9.3% | 9.2% | 17.3% | 7.8% | 21.4% | 8.9% | 14.7% | 9.8% | 15.8% | 9.1% |
| 7-12 months | 18.7% | 4.8% | 8.8% | 10.7% | 15.9% | 7.3% | 25.2% | 9.4% | 16.5% | 9.7% | 12.9% | 9.6% |
| 13-18 months | 22.0% | 4.8% | 10.3% | 9.1% | 16.3% | 7.2% | 17.5% | 8.3% | 15.9% | 7.5% | 10.6% | 8.6% |
| 19-24 months | 22.3% | 4.3% | ND | 11.4% | 20.5% | 6.8% | 18.7% | 10.8% | 15.4% | 7.9% | 13.3% | 10.3% |
| 25-30 months | 15.1% | 3.6% | ND | 11.1% | 15.3% | 5.8% | 18.1% | 10.0% | 16.1% | 7.9% | ND | 9.1% |
| 31-36 months | 15.7% | 3.8% | ND | 10.2% | 21.9% | 6.1% | ND | 7.6% | 13.5% | 7.7% | ND | 9.1% |
| TANF | ||||||||||||
| 1-6 months | 2.3% | 0.7% | 3.9% | 1.4% | 9.4% | 2.8% | 3.4% | 1.8% | 2.1% | 1.0% | 0.0% | 1.9% |
| 7-12 months | 3.0% | 0.6% | 3.7% | 1.5% | 8.7% | 2.5% | 6.6% | 1.5% | 3.8% | 0.9% | 1.3% | 1.9% |
| 13-18 months | 5.3% | 0.5% | 6.8% | 1.4% | 5.8% | 1.9% | 10.1% | 1.3% | 3.6% | 0.7% | 3.1% | 1.5% |
| 19-24 months | 3.7% | 0.5% | ND | 1.8% | 3.1% | 1.7% | 7.9% | 2.1% | 1.7% | 0.8% | 4.3% | 1.6% |
| 25-30 months | 0.7% | 0.4% | ND | 3.4% | 4.3% | 1.4% | 3.9% | 1.5% | 1.4% | 0.4% | ND | 1.3% |
| 31-36 months | 0.8% | 0.4% | ND | 2.4% | 6.1% | 1.4% | ND | 1.1% | 0.0% | 0.0% | ND | 0.5% |
| SSI Benefits | ||||||||||||
| 1-6 months | 0.5% | 1.3% | 0.0% | 6.3% | 0.9% | 3.8% | 1.9% | 2.0% | 0.9% | 3.3% | 1.4% | 5.1% |
| 7-12 months | 3.1% | 1.5% | 1.1% | 7.0% | 2.5% | 3.9% | 1.9% | 2.5% | 2.3% | 3.8% | 1.8% | 7.1% |
| 13-18 months | 5.2% | 1.9% | 1.0% | 5.9% | 1.4% | 4.2% | 2.2% | 2.7% | 1.5% | 4.0% | 1.9% | 7.0% |
| 19-24 months | 5.1% | 2.0% | ND | 7.9% | 2.7% | 4.8% | 2.5% | 2.7% | 1.0% | 4.5% | 1.9% | 9.5% |
| 25-30 months | 6.8% | 2.6% | ND | 8.6% | 8.8% | 6.1% | 3.4% | 3.7% | 5.1% | 5.6% | ND | 8.2% |
| 31-36 months | 4.2% | 2.5% | ND | 13.8% | 12.1% | 6.5% | ND | 5.4% | 10.3% | 12.9% | ND | 8.4% |
| Employer-Based Disability Insurance | ||||||||||||
| 1-6 months | 3.4% | 0.3% | 72.7% | 72.0% | 3.6% | 0.8% | 4.3% | 2.0% | 4.9% | 1.6% | 2.5% | 3.5% |
| 7-12 months | 4.4% | 0.3% | 35.2% | 28.0% | 1.9% | 1.0% | 4.1% | 1.5% | 5.2% | 2.1% | 4.6% | 2.6% |
| 13-18 months | 3.6% | 0.4% | 23.0% | 16.7% | 3.3% | 1.0% | 3.3% | 0.6% | 6.0% | 2.4% | 6.0% | 2.1% |
| 19-24 months | 3.7% | 0.5% | ND | 14.2% | 5.9% | 1.1% | 4.4% | 1.2% | 5.9% | 2.6% | 9.3% | 4.4% |
| 25-30 months | 5.6% | 0.5% | ND | 16.4% | 8.4% | 0.6% | 1.4% | 1.6% | 5.6% | 2.8% | ND | 2.2% |
| 31-36 months | 1.7% | 0.4% | ND | 15.4% | 10.3% | 0.4% | ND | 1.0% | 9.7% | 4.3% | ND | 1.3% |
| Workers' Compensation | ||||||||||||
| 1-6 months | 2.8% | 1.1% | 6.7% | 10.3% | 7.0% | 4.2% | 2.5% | 4.0% | 10.5% | 4.9% | 90.8% | 89.8% |
| 7-12 months | 3.7% | 1.0% | 6.1% | 8.8% | 7.7% | 3.6% | 4.3% | 3.3% | 11.9% | 5.3% | 66.3% | 39.8% |
| 13-18 months | 4.8% | 0.8% | 9.0% | 6.8% | 6.2% | 3.2% | 2.2% | 2.6% | 11.3% | 3.6% | 47.3% | 22.6% |
| 19-24 months | 3.5% | 0.6% | ND | 6.0% | 6.5% | 2.3% | 3.1% | 2.5% | 14.0% | 3.6% | 41.8% | 18.1% |
| 25-30 months | 3.7% | 0.8% | ND | 4.7% | 6.3% | 2.5% | 2.2% | 1.1% | 10.8% | 3.0% | ND | 13.3% |
| 31-36 months | 3.9% | 0.9% | ND | 3.8% | 4.8% | 2.6% | ND | 1.3% | 6.9% | 3.4% | ND | 6.5% |
| Medicaid | ||||||||||||
| 1-6 months | 12.2% | 6.9% | 14.9% | 18.3% | 18.2% | 11.9% | 16.5% | 15.0% | 12.9% | 14.4% | 17.0% | 17.7% |
| 7-12 months | 19.6% | 6.9% | 14.9% | 20.1% | 17.4% | 12.0% | 26.1% | 15.0% | 16.8% | 14.7% | 16.9% | 20.6% |
| 13-18 months | 27.3% | 6.8% | 19.1% | 19.5% | 20.3% | 10.6% | 29.5% | 13.9% | 15.2% | 13.5% | 22.6% | 19.9% |
| 19-24 months | 30.3% | 6.5% | ND | 19.4% | 24.0% | 10.7% | 28.8% | 15.7% | 16.4% | 14.3% | 26.6% | 19.3% |
| 25-30 months | 32.5% | 5.7% | ND | 17.5% | 21.3% | 11.0% | 26.8% | 14.4% | 12.6% | 14.1% | ND | 12.5% |
| 31-36 months | 28.5% | 5.2% | ND | 19.6% | 27.4% | 11.5% | ND | 15.1% | 23.9% | 15.6% | ND | 13.9% |
| Private Health Insurance | ||||||||||||
| 1-6 months | 68.9% | 81.1% | 89.4% | 79.3% | 74.1% | 81.6% | 62.2% | 68.2% | 69.3% | 71.8% | 67.8% | 69.7% |
| 7-12 months | 62.0% | 80.4% | 87.5% | 77.9% | 71.9% | 82.3% | 59.5% | 69.4% | 70.5% | 74.8% | 70.9% | 69.1% |
| 13-18 months | 58.8% | 80.4% | 79.2% | 79.2% | 73.3% | 82.2% | 63.1% | 65.8% | 71.4% | 73.2% | 71.6% | 66.7% |
| 19-24 months | 60.1% | 81.1% | ND | 80.4% | 65.8% | 82.4% | 67.4% | 68.4% | 72.5% | 76.7% | 68.2% | 70.7% |
| 25-30 months | 65.6% | 79.2% | ND | 71.4% | 70.4% | 82.4% | 58.7% | 68.6% | 66.2% | 74.8% | ND | 71.1% |
| 31-36 months | 57.6% | 80.4% | ND | 72.8% | 71.0% | 83.1% | ND | 70.5% | 67.2% | 80.7% | ND | 65.6% |
| Household Income | ||||||||||||
| 1-6 months | $2,636 | $3,598 | $4,854 | $4,901 | $4,241 | $5,117 | $3,078 | $3,870 | $3,408 | $4,187 | $3,672 | $4,784 |
| 7-12 months | $2,623 | $3,889 | $4,577 | $4,653 | $4,204 | $5,092 | $2,960 | $3,825 | $3,433 | $4,276 | $3,760 | $4,425 |
| 13-18 months | $2,673 | $3,941 | $4,165 | $4,655 | $4,286 | $5,353 | $3,029 | $3,742 | $3,223 | $4,248 | $3,673 | $4,506 |
| 19-24 months | $2,794 | $4,149 | ND | $5,087 | $4,346 | $5,271 | $3,037 | $3,862 | $3,570 | $4,189 | $3,533 | $4,771 |
| 25-30 months | $2,767 | $3,893 | ND | $5,548 | $3,575 | $5,391 | $3,002 | $3,888 | $3,304 | $4,129 | ND | $4,903 |
| 31-36 months | $2,668 | $3,997 | ND | $4,994 | $3,702 | $5,474 | ND | $3,660 | $3,273 | $4,565 | ND | $4,554 |
| Individual Earnings | ||||||||||||
| 1-6 months | $1,192 | $1,792 | $1,187 | $1,276 | $1,637 | $2,469 | $1,337 | $1,636 | $1,101 | $1,617 | $656 | $1,341 |
| 7-12 months | $1,003 | $1,966 | $1,037 | $1,542 | $1,549 | $2,456 | $1,150 | $1,575 | $964 | $1,668 | $640 | $1,451 |
| 13-18 months | $921 | $1,968 | $948 | $1,612 | $1,390 | $2,567 | $1,223 | $1,531 | $905 | $1,672 | $580 | $1,666 |
| 19-24 months | $956 | $2,099 | ND | $2,010 | $1,196 | $2,481 | $1,176 | $1,560 | $945 | $1,675 | $767 | $1,889 |
| 25-30 months | $963 | $1,952 | ND | $2,392 | $1,147 | $2,536 | $1,117 | $1,589 | $714 | $1,630 | ND | $1,803 |
| 31-36 months | $939 | $2,004 | ND | $1,674 | $870 | $2,599 | ND | $1,473 | $772 | $1,845 | ND | $1,599 |
| Individual Earnings of Those with Earnings | ||||||||||||
| 1-6 months | $2,474 | $1,903 | $2,624 | $2,690 | $2,154 | $2,894 | $1,551 | $1,779 | $2,119 | $2,755 | $1,791 | $2,759 |
| 7-12 months | $2,644 | $1,769 | ND | $2,945 | $2,348 | $2,930 | $1,481 | $1,819 | $2,120 | $2,760 | $2,373 | $2,682 |
| 13-18 months | $2,659 | $1,801 | ND | $2,745 | $2,113 | $3,072 | $1,590 | $1,804 | $2,042 | $2,767 | ND | $2,966 |
| 19-24 months | $2,775 | $1,987 | ND | $3,245 | $2,034 | $3,009 | $1,606 | $1,879 | $2,044 | $2,720 | ND | $3,054 |
| 25-30 months | $2,615 | $2,059 | ND | $3,889 | ND | $3,029 | $1,584 | $1,985 | ND | $2,708 | ND | $2,923 |
| 31-36 months | $2,680 | $2,079 | ND | ND | ND | $3,130 | ND | $1,772 | ND | $2,948 | ND | $2,741 |
| Individual Income | ||||||||||||
| 1-6 months | $1,476 | $2,015 | $2,788 | $2,367 | $1,968 | $2,759 | $1,499 | $1,807 | $1,751 | $2,224 | $1,627 | $2,314 |
| 7-12 months | $1,315 | $2,192 | $2,173 | $2,243 | $1,932 | $2,754 | $1,377 | $1,810 | $1,695 | $2,241 | $1,620 | $2,030 |
| 13-18 months | $1,321 | $2,197 | $1,721 | $2,264 | $1,862 | $2,868 | $1,492 | $1,790 | $1,653 | $2,302 | $1,460 | $2,145 |
| 19-24 months | $1,352 | $2,348 | ND | $2,704 | $1,711 | $2,792 | $1,520 | $1,846 | $1,777 | $2,334 | $1,434 | $2,399 |
| 25-30 months | $1,429 | $2,184 | ND | $3,155 | $1,664 | $2,887 | $1,492 | $1,838 | $1,659 | $2,303 | ND | $2,252 |
| 31-36 months | $1,470 | $2,212 | ND | $2,252 | $1,548 | $2,981 | ND | $1,722 | $1,592 | $2,391 | ND | $2,033 |
| SOURCE: 1996, 2001, and 2004 SIPP panels matched to SSA administrative data. NOTES: Table is illustrative of program participation and incomes of at-risk group members in 6-month intervals after they were identified in the at-risk group. Bold type indicates values of SSDI applicants and non-applicants that are significantly different at p<0.05. ND = no data (sample size fewer than 50). | ||||||||||||
We show participation in selected programs and incomes in Table IV.7. While individuals who eventually applied for SSDI tended to have higher rates of program participation than those who did not, as expected, these differences were often not significantly different, which in part is due to the small sample sizes for each group. The consistency in the patterns observed across at-risk groups, though, is important. Individuals who later applied for SSDI benefits in all groups except for private disability insurance and workers' compensation generally had higher levels of SNAP and Temporary Assistance for Needy Families (TANF) benefits. SSDI applicants with high health expenditures or who were veterans with disabilities initially had higher levels of employer-based disability benefits and workers' compensation. SSDI applicants in the high health expenditure group had consistently higher levels of Medicaid and lower levels of private health coverage than those who were not. Among workers' compensation group members, SSDI applicants generally had higher rates of workers' compensation benefit receipt over time, suggesting that these individuals had more severe or long-lasting conditions that qualified them for workers' compensation benefits; we did not observe a similar pattern for private disability insurance members regarding employer-based or individual disability benefits. SSDI applicants typically had lower earned incomes than non-applicants, and income fell over time, while income of non-applicants remained stable or increased. Regarding individual and household income measures, non-applicants had stable or increasing incomes, whereas SSDI applicants had stable or decreasing incomes; these patterns were not consistent, however, and varied across groups.
4. Conclusion
In this chapter, we examined the employment and program-participation paths of individuals with disabilities who did and did not apply for SSDI. The patterns help us understand the characteristics of those at greater risk of SSDI entry compared to those who do not enter SSDI, most of whom continued working. This can help craft policies that simultaneously divert those with disabilities from applying for SSDI while providing the support necessary to make work feasible for those with disabilities.
As expected, we observed a decline in employment and earned income of SSDI applicants before applying for benefits, with the biggest change observed in the six months immediately preceding SSDI application. However, somewhat surprisingly, a large share of these individuals (more than two-thirds) was employed at some point during this period; similarly (and somewhat related), most SSDI applicants had private health insurance coverage. A larger proportion of eventual SSDI applicants received poverty-related benefits up to 42 months before applying for SSDI than individuals in the general population, and participation in these benefits programs showed an increase during the six months immediately before SSDI application.
Among individuals in at-risk groups, those with private disability insurance had the highest rates of applying for SSDI. At-risk group members who applied for SSDI were more likely to participate in various programs than at-risk group members who did not apply for SSDI, though the patterns varied by the at-risk group.
This analysis uncovers key patterns for SSDI applicants and non-applicants, but two important caveats bear mentioning. First, sample sizes are quite small for a few of the programs included in our study, so drawing conclusions regarding the pathways from these programs to SSDI application is limited. Second, data regarding disability status is not available during each SIPP wave, which makes it difficult to determine the disability status of individuals participating in certain programs.
Future research should further investigate the various paths to SSDI application and receipt. One area could focus on individuals with specific disabilities to gain a more nuanced understanding of the factors that lead to SSDI application and continued participation in the labor market. Additionally, uncovering the eventual SSDI application decisions of those with disabilities who participate in VR and RTW initiatives would be instructive.
V. Funding for Employment-related Services and Supports for People with Psychiatric Disorders and Other Disabilities
A. Introduction
In this chapter, we review current funding mechanisms for SE and other employment supports for people with psychiatric disorders and other disabilities. The chapter is divided into two sections. In Section B, we review funding for SE and other employment supports available through Medicaid. In Section C, we review other funding sources for employment supports, such as state VR agencies, America's Career Centers Network, the VA, and employer-sponsored programs. Because individual agencies restrict the types of activities they fund, states often "braid" together funding from multiple sources to deliver comprehensive evidence-based SE programs. The major funding sources for employment supports are public, and many are limited to individuals eligible for Medicaid. Because individuals' incomes increase once they are successfully employed, they may lose eligibility for these supports, jeopardizing their ability to maintain employment. Moreover, such funding sources are of limited use for preventing unemployment and disability among people with psychiatric disorders who are not yet disabled. Several provisions of the ACA, discussed in the next chapter, are particularly important for preventing unemployment and disability and supporting working people with disabilities.
B. Medicaid Funding for Employment-Related Services and Supports for Individuals with Psychiatric Disorders and Other Disabilities
Medicaid provides several opportunities for funding employment services for people with psychiatric disorders and other disabilities; the specific eligibility requirements for each vary. In this section, we provide information on the various options, including waivers, State Plan Options, demonstrations, and the Medicaid Buy-In.
1. Medicaid 1915(c) HCBS Waiver
Section 1915(c) of the Social Security Act authorizes a waiver program that allows states to provide home and community-based services (HCBS) to persons who, but for the provision of HCBS, would require an institutional level of care. Although these funds can be used for people with mental illness, they typically are not. Programs funded through 1915(c) waivers are required to be budget neutral (Karakus et al. 2011), meaning that HCBS costs must offset Medicaid institutional costs that would have been incurred if the person had been institutionalized. Medicaid reimbursement is currently denied for individuals ages 21-64 if they reside in institutions for mental disease (IMDs), making Medicaid cost-neutrality difficult to achieve (Bazelon Center 2012b).
Although 1915(c) waiver funding cannot be used for vocational services that are delivered in "facility-based or sheltered work settings," it can be used for pre-vocational services, including "vocational/job-related discovery or assessment, person-centered employment planning, job placement, job development, negotiation with prospective employers, job analysis, job carving, training and systematic instruction, job coaching, benefits support, training and planning, transportation, asset-development and career advancement services, and other workplace support services, including services not specifically related to job skill training that enable the waiver participant to be successful in integrating into the job setting" (HHS 2011).
2. Medicaid 1915(i) HCBS State Plan Option
Added to the Social Security Act by the Deficit Reduction Act (DRA) of 2005, section 1915(i) is a state-plan option that can be used to provide services similar to those available through 1915(c) waivers. Unlike with 1915(c) however, states must demonstrate that the needs-based criteria for receiving 1915(i) services are less stringent than the criteria for meeting an institutional level of care. The 1915(c) cost-neutrality requirement does not exist with this option (Bazelon Center 2012b), and that expands the opportunity for states to fund employment-related services, including SE, for people with psychiatric disabilities. Elements of supported education that are integrated into SE and provided directly to the individual, as opposed to general outreach to educational institutions, can be funded under Section 1915(i). States can cover these services through a state plan amendment, which may also be less burdensome for states to obtain than a waiver.15, 16
3. Medicaid 1915(b)(3) Managed Care Delivery System Waiver
Under the 1915(b)(3) waiver, states can enroll eligible individuals into Medicaid managed care plans. This waiver permits states to use the cost savings achieved through managed care to provide additional services--known as "reinvestment services"--to Medicaid recipients (Fields n.d.). Reinvestment services can include all components of SE. In Washington, for example, funds gained through the waiver are used for a range of SE services, including an individual assessment of skills, training, and education; resume development and interview preparation; creation of individualized job and career-development plans; assistance in locating employment opportunities; and outreach/job coaching at a worksite. Waiver funds can also be used to supplement other funding streams. For example, funds to provide VR services through Title I of the Rehabilitation Act (described in Chapter III) may be used to provide SE until an individual reaches the 18-month limit, at which point 1915(b)(3) waiver funds can be used to continue services (Karakus et al. 2011).
4. Medicaid Rehabilitation Services Option--Section 1905(a)(13)
The Medicaid Rehabilitation Option (Rehab Option) is available to cover services that help individuals with daily living, interpersonal, and communication skills (Smith et al. 2005). It allows states to cover "diagnostic, screening, preventive, and rehabilitative services (provided in a facility, a home, or other setting) recommended by a physician or other licensed practitioner for the maximum reduction of physical or mental disability and restoration of an individual to the best possible functional level."17 States use the Rehab Option to offer a number of services to individuals with SMI (Fields n.d.; Karakus et al. 2011). Although states vary in the scope of services they offer under the Rehab Option, a 2005 handbook issued by HHS states that "a full-featured, comprehensive coverage of rehabilitative services for individuals with SMI will include: peer support, life skills training and support across a variety of community living dimensions and SE" (Smith et al. 2005).
The statutory and regulatory provisions surrounding the Rehab Option are brief and somewhat vague. One directive that is clearly stated, however, is that "habilitative" services cannot be funded using this option, but "rehabilitative" can. Rehabilitative services are designed to be restorative or remedial services provided to an individual who has a condition that has resulted in a loss of functioning; habilitative services help individuals to initially acquire new skills (Smith et al. 2005). To be funded under the Rehab Option, states must ensure that SE services for people with SMI and other disabilities meet the definition of "rehabilitative" services.
In 1992, the Health Care Financing Administration (now CMS) issued guidance to states on how to use the Rehab Option for those with SMI (Health Care Financing Administration 1992). The letter stated that "while it is not always possible to determine whether a specific service is rehabilitative by scrutinizing the service itself, it is more meaningful to consider the goal of the treatment. Services necessary for the treatment of mental illness may be coverable as rehabilitative services." However, the same letter also gave examples of services that did not fall under the definition of rehabilitation, one of which was "vocational training: job training, vocational, and education services." In its analysis of this letter, the 2005 HHS handbook notes that "this prohibition does not preclude the provision of services that might assist individuals to function in the workplace, provided that the services furnished are not directly associated with specific job performance" (Smith et al. 2005). Therefore, funds from the Rehab Option may be used to pay for parts of SE programs, such as peer support, training in social skills, or counseling. However, certain vocational services (such as teaching particular skills needed for a specific job, or assistance with a job search) are excluded under this option (Fields n.d.). The Rehab Option can also be used to cover assertive community treatment (Smith et al. 2005), which, in its full fidelity evidence-based model, includes an employment specialist and may provide full fidelity evidence-based SE.
5. Medicaid Targeted Case Management State Plan Amendment
Targeted case management (TCM) is used by states to provide case management to targeted groups of Medicaid-eligible individuals (Binder 2008), which could include individuals with disabilities. TCM can be used to help the targeted group gain access to medical, education, and other services, regardless of whether the services in question are covered by Medicaid (Fields n.d.). Case managers can conduct activities to help individuals gain employment, including assessment of the individual to determine needs for social, medical, or other services; developing a treatment plan that outlines case management goals and an action plan to respond to the individual's needs; referrals and other similar activities to help the person access the service in his or her plan (or other services that will further the achievement of personal goals, including employment services); and monitoring the care plan to ensure that it is effectively implemented and that needs are addressed (Karakus et al. 2011; Smith et al. 2005). TCM funds could, therefore, be used to pay for parts of SE programs.
6. Money Follows the Person Demonstration
Through the CMS Money Follows the Person (MFP) Demonstration, 44 states have received federal grants to transition Medicaid beneficiaries from institutions to home or community settings. Originally enacted in 2006, the demonstration program offers state Medicaid programs an enhanced federal match for each enrollee who successfully transitions out of an institutional setting. In recent years, 24 states have taken steps to increase the number of individuals with SMI and other disabilities who transition out of institutions under the MFP demonstration (O'Malley Watts 2011).
The MFP demonstration is intended to shift Medicaid funding from institutions to community-based settings, remaining cost-neutral in the process. Because Medicaid prohibits spending on care for individuals ages 21-64 with mental illness residing in IMDs, cost-neutrality is harder to demonstrate with this population. Some states (including Delaware and Pennsylvania), therefore, have not included individuals with mental illness in this age range in their MFP demonstrations. However, states are able to include costs of care for individuals with mental illnesses who reside in nursing homes and psychiatric units in general hospitals as potential cost offsets to demonstrate cost-neutrality. Connecticut administers a MFP behavioral health initiative that combines MFP funds with a 1915(c) waiver. Through this program, the state offers a range of services to adults 22 years old and older who are Medicaid-eligible; meet Medicaid State Plan criteria for nursing home level of care; have a diagnosis of SMI; and are either a resident of a nursing facility, an MFP participant, or have a psychiatric history, impairment, and service needs. SE is included in the services provided to MFP participants. However, any services under MFP to those with mental illness can be provided only to individuals transitioning out of nursing homes, not to those in IMDs, thereby inherently limiting the usefulness of this source of funding for this population (Prewitt et al. 2011; Connecticut Department of Mental Health & Addiction Services 2012).18
7. Continued Medicaid Eligibility Work Incentive--Section 1619(b) of the Social Security Act--and the Medicaid Buy-In
Two options enable workers to retain Medicaid coverage as their earnings increase. Although they do not fund SE and employment services, they do enable beneficiaries to retain valuable medical coverage as their earnings rise. Section 1619(b) of the Social Security Act provides for continued Medicaid eligibility for employed SSI beneficiaries to provide an incentive to work (SSA n.d.). To remain eligible for Medicaid while working, an individual must have been eligible for an SSI payment for at least one month; still meet the disability requirement and all other SSI requirements; demonstrate that he or she needs Medicaid benefits to continue to work; and have gross earnings that are too low to replace SSI, Medicaid, and any publicly funded personal care services the individual receives. The Medicaid Buy-In program, authorized by the Balanced Budget Act of 1997 and the Ticket to Work and Work Incentives Improvement Act (Ticket Act) of 1999, provides another opportunity for employed adults with disabilities to maintain Medicaid coverage and earn more than the income limits. Individuals may "buy in" to the program by paying premiums that are determined by their income. Both programs may be attractive to individuals with disabilities who meet the SSA definition of disability but who have high enough earnings that they would otherwise be ineligible for Medicaid.
C. Other Sources of Funding for Employment Supports
Several federal agencies also offer sources of funding that may be used to directly provide SE to individuals with mental illness or otherwise encourage them to work. These include various block grants, VR and special education programs, VA services, and other demonstrations.
1. SAMHSA's Community Mental Health Services Block Grant
CMHS Block Grant funds, administered by SAMHSA, can be used to pay for aspects of SE programs, including mental health treatment and vocational services, for individuals with SMI (Bazelon Center 2010; Karakus et al. 2011). Block Grant funds can be used to establish new mental health programs and services, build on existing programs, increase access to community-based services, and leverage additional funding from state or community sources (Altarum Institute 2010b). Each state must submit an application detailing how it will use the funds to create an organized, community-based system of care for individuals with mental illness. Block Grant funds are extremely flexible and can be used to pay for aspects of SE that cannot be paid for by other funding sources. For example, they can be used to pay for indirect services, such as clinical supervision, fidelity assessments, training, and integrated staff meetings that are necessary for maintaining fidelity to the evidence-based SE model that cannot be covered through Medicaid (which can pay only for direct services to the beneficiary). All 50 states and the District of Columbia receive Block Grant funding (SAMHSA 2012).
2. RSA's VR Services Program and SE State Grants (VI-B State Grants)
RSA provides several types of grants to states to fund employment programs for individuals with disabilities. This source of employment support may be important for individuals who are ineligible for Medicaid. In addition to the VR services described in Chapter III, the RSA provides grants to state VR agencies specifically for SE services. These grants are intended to supplement VR state grants. Known as Supported Employment for Individuals with the Most Significant Disabilities Title VI-B State Grants, they are meant to help states develop collaborative programs with various entities to provide SE services to individuals with severe disabilities.19 SE must be determined to be an appropriate rehabilitation objective for that individual based on a comprehensive rehabilitation-needs assessment.20 Services covered include: (1) any additional assessment needed; (2) development of job placements; and (3) provision of services needed to support individuals in their jobs, such as intensive on-the-job skills and other training needed to maintain job stability, follow-up, and such post-employment services as job-station re-design.21 However, funds "cannot be used to provide the extended services necessary to maintain individuals in employment after the end of SE services, which usually do not exceed 18 months" (U.S. Department of Education n.d. a).
3. Individuals with Disabilities Education Act Funding for SE
The Individuals with Disabilities Education Act requires that an Individualized Education Program (IEP) be developed for students in special education if it is needed to help the student participate to his or her maximum potential. The IEP specifies the services that must be provided and funded by the school district and must be tailored to the individual's needs, as identified through an evaluation process. Transition services must be provided to help the student move from school to employment or further education. SE may be specified in the IEP as a transition service. However, we were unable to identify the extent to which SE is provided to individuals with SMI through IEPs.
4. Employment and Training Administration's America's Job Center Network
The America's Job Center Network (formerly called One-Stop Career Centers) was established under the Workforce Investment Act to provide comprehensive assistance to job seekers. Services offered by these centers include training referrals, career counseling, and access to job listings. Because America's Job Centers offer general support services rather than services that are specific to mental health or disability, they may be more appealing to young people or others for whom stigma is an issue. They are also especially useful for people with mental illnesses who are not yet disabled or do not qualify for disability benefits. America's Job Centers have been used by some states to provide employment assistance to people with disabilities, though questions remain about whether they are equipped to provide services to individuals with SMI (Karakus et al. 2011). In a 2009 survey of One-Stop Career Center staff in several states, respondents reported seeing a greater number of customers with mental health issues during the recession years of 2007-2009 (Heidkamp & Mabe 2011). To better serve these individuals, center staff in several states said they were connecting their services to mental and behavioral health systems.
5. U.S. Department of Veterans Affairs' VR, Compensated Work Therapy, and Homeless Veterans Supported Employment Programs
The VA provides a number of employment services for qualifying veterans through the Vocational Rehabilitation and Employment (VR&E) program, Compensated Work Therapy, and the Homeless Veterans Supported Employment Program. The VR&E program offers employment supports to veterans who have service-connected disabilities. Services available under this program include an evaluation to determine skills, abilities, and interests; vocational counseling and planning for employment services; various employment services, such as job training and development of job-search skills and resumes; assistance finding and keeping a job, including incentives to employers and special job accommodations; on-the-job training and apprenticeships; training at a college, vocational, or technical school; and case management, counseling, and medical referrals.
Through Compensated Work Therapy, the VA offers VR programs, including SE, which seek to place veterans in jobs (U.S. Department of Veterans Affairs 2009). The SE Program helps veterans with disabilities identify and obtain jobs based on individualized preferences and then provides ongoing support and vocational assistance (Resnick & Rosenheck 2007). The Homeless Veteran SE Program offers SE to homeless veterans and those who are at risk of homelessness (U.S. Department of Veterans Affairs n.d.).
6. SSA's TTW Program
The TTW program, also described in Chapter III, enables any state VR agency, America's Job Center, or mental health provider (including a consumer-operated or peer-service provider) to become an employment network (EN) and provide employment-support services. An EN receives payments if it helps the beneficiary achieve earnings high enough to reduce or eliminate SSA cash benefits (Altshuler et al. 2011). TTW funds, therefore, can be used to fund any aspect of SE programs. However, few ENs provide the intensive support that beneficiaries with significant disabilities need to sustain the level of employment required for the EN to receive payment.
TTW funds can be used concurrently with 1915(c) waiver funds to create more comprehensive SE programs. Because TTW payments are made based on employment-related outcomes and milestones achieved by beneficiaries (rather than on a cost-reimbursement basis), CMS has determined that using them together with waiver funds does not constitute an overpayment of federal dollars (HHS 2011).
Work Incentives Planning and Assistance programs, also authorized by the Ticket Act, advise Social Security disability beneficiaries on how to use work incentives available through Social Security disability benefits programs. Work incentives counseling is now one of the core components of SE, and many SE providers have become certified work incentives counselors.
7. Employer-Sponsored Employment-Support Services
Employers fund DM through their own funds, or through private insurance carriers that provide workers' compensation or short-term or long-term disability insurance. The companies that have successfully reduced costs take an active role in managing their work-injury cases. Companies use this case management function--formally or informally--whether they are commercially insured and receive claim management assistance from its carrier or they use a medical management group to provide RTW services.
SE is not typically covered under private health insurance, but some employers may include some aspects of it under short-term or long-term disability insurance, DM, or company-sponsored employment assistance programs. However, access to employee-sponsored DM programs is important for individuals who are not covered by Medicaid, because their income is too high or because they do not meet the eligibility criteria for Social Security disability benefits.
VI. Opportunities for Funding Supported Employment and Other Employment Supports Under the Affordable CARE ACT
A. Introduction
In this chapter, we describe provisions of the ACA that extend health insurance coverage and increase access to appropriate services to individuals with disabilities, including psychiatric disorders. The ACA contains a number of provisions that have the potential to impact individuals with disabilities and their ability to seek or maintain employment. We also detail the possible challenges individuals may experience as they transition from Medicaid to other insurance programs when their earnings change--a circumstance that might be expected to affect populations with SMI and other disabilities.
B. Elements of the Affordable Care Act That Might Affect Individuals with Psychiatric Disorders and Other Disabilities
Individuals with psychiatric disorders and other disabilities frequently require ongoing medical treatment, mental health services, in-home assistance, and other support to secure and maintain employment. Health insurance is, therefore, a critical factor regarding their ability to work. Some aspects of the ACA might help this population gain insurance through public or private channels, as outlined below.
1. The Medicaid Expansion and Health Insurance Exchanges
Beginning in January 2014, the ACA provides federal funding for states that choose to expand Medicaid eligibility to include individuals with incomes up to 133 percent of the FPL, regardless of disability or parental status. A 5 percent income disregard established in the ACA effectively raises this limit to 138 percent of the FPL (HHS, CMS n.d.). The Medicaid expansion is likely to have an important effect on the ability of people with disabilities with low and moderate income, but who are not eligible or who do not meet the definition of disability for SSI or SSDI, to obtain health insurance. The effect will vary by state,however, as the Supreme Court has ruled that each state can decide whether to expand its Medicaid program (Musumeci 2012).
In all states, individuals can purchase insurance through health insurance exchanges with open enrollment beginning October 1, 2013 (HHS n.d.). In 2014, premium tax credits became available to help those with incomes between 100 percent and 400 percent of the FPL afford insurance through these exchanges if they are not eligible for coverage through their employer or through public programs. Even individuals who are eligible for coverage through an employer can receive premium tax credits if the employer's share of the cost of coverage is less than 60 percent or if the premium for individual coverage is more than 9.5 percent of the person's income. In addition, cost-sharing subsidies are available--through deductibles, co-pays, or co-insurance--to individuals with incomes at or below 250 percent of the FPL to help limit out-of-pocket costs (Kaiser Family Foundation 2012). These provisions could allow people with psychiatric disorders or other disabilities who do not qualify for Medicaid to purchase insurance on their own, regardless of employment status.
In states that do not expand their Medicaid programs, those who are ineligible for Medicaid but remain below 100 percent of the FPL cannot receive premium tax credits and will likely be unable to afford private insurance (Kaiser Family Foundation 2012). Approximately two-thirds of the people who would have been eligible for Medicaid if the expansion had been nationwide will have income too low to qualify for exchange subsidies (Congressional Budget Office 2012).
2. Expanded Availability of Mental Health Services Through Public and Private Insurance Coverage
Before the ACA, the Mental Health Parity Act of 1996--together with the Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act (MHPAEA) of 2008--created the nation's federal mental health parity requirements (Sarata 2011). Neither of these laws mandated that insurers offer mental health benefits. Rather, they required that employers choosing to offer these benefits provide them at levels similar to medical and surgical benefits. The Mental Health Parity Act of 1996 forbade group health insurance plans--defined as those with more than 50 employees--from placing annual and lifetime dollar limits on mental health benefits that were less than those placed on medical and surgical benefits. The MHPAEA prohibits group insurance plans from imposing financial requirements (such as co-insurance, deductibles, or co-payments) or treatment limitations on mental health benefits in a more restrictive way than these requirements or limitations are imposed on most medical or surgical benefits. It also extends these parity requirements to services for substance use disorders, and requires parity in in-network and out-of-network benefits (Sarata 2011; SAMHSA 2011).
Until the enactment of the ACA, coverage of mental health and substance use disorder benefits by private insurers remained optional. In addition, the federal parity law applied only to large group insurance plans. The ACA, however, requires that any insurance package offered in the individual or small-group markets, both inside and outside of the exchanges, cover certain categories of services, known as the "essential health benefits" (EHB) (Kaiser Family Foundation 2013; HHS 2012).22 Services for mental health and substance use disorders, provided in compliance with federal parity requirements, are included in the list of required benefits. Further, in implementing the EHB provisions of the ACA, HHS has finalized regulations that apply federal parity requirements to the mental health and substance use disorder benefits that both small-group and individual plans must include as part of the EHB requirements (Beronio et al. 2013).23
However, HHS has allowed states significant latitude in defining the scope of benefits (Siegwarth & Koyanagi 2012). States are required to select a "benchmark" plan that may be: "(1) the largest plan by enrollment in any of the three largest products in the state's small-group market; (2) any of the largest three state employee health benefit plans options by enrollment; (3) any of the largest three national Federal Employees Health Benefits Program plan options by enrollment; or (4) the largest insured commercial HMO in the state" (HHS 2012). The scope of benefits available under the selected plan then serves as the "benchmark" for plans in that state offered through the insurance exchange. If the selected plan does not include any of the essential benefits required under the ACA, states must supplement the plan by adding the entire category of benefits from another benchmark plan that does include those services. Additionally, strong non-discrimination language in the law ensures that plans will be designed in a way that prevents insurers from making decisions about coverage, reimbursement rates, establishing incentive programs, and designing benefits based on degree of disability or health conditions. This is highly relevant for mental health services, as employer plans do not always offer this category of service (Siegwarth & Koyanagi 2012). Even with the introduction of health insurance exchanges, however, it remains unlikely that many private insurance plans will provide employment supports to their members. It will become even more important to understand how public sources of funding can be used to provide employment supports to people with psychiatric disorders.
In addition to their application in the design of EHBs, "benchmark" plans are also relevant for the Medicaid expansion population. States are not required to offer their full Medicaid plans to the newly eligible, but may instead offer a plan that simply meets the benchmark requirements established in section 1937 of the Social Security Act, supplemented as necessary to meet the ACA's EHB requirements (for example, adding coverage for substance use disorders if not already included in the benchmark plan [Siegwarth & Koyanagi 2012]). These alternative benefit plans, as CMS has termed them, must also meet the federal parity requirements. As long as these requirements are met, states may provide a different benefit package for new Medicaid beneficiaries. However, some groups are considered exempt; they cannot be required to enroll in the alternative benefit plans and are entitled to all covered Medicaid services which sometimes include SE (Bazelon Center 2012b; Siegwarth & Koyanagi 2012). Federal regulations include "individuals with disabling mental disorders" and "individuals with physical and/or mental disabilities that significantly impair their ability to perform one or more activities of daily living," within the exempt category of medically frail and special-needs populations. Individuals with mental illness outside of the aforementioned two categories are not exempt from enrollment in limited benefit plans (42 CFR § 440.315(f)).24
Although states may choose to provide an alternative benefit package to newly eligible adults, they have the option of providing their full Medicaid package to these individuals using the benchmark option of "secretary approved coverage." Additionally, states may provide different benchmark packages targeted to different populations, so they can, if they wish, tailor benefits, including employment-support needs25 to meet the unique needs of individuals with mental illnesses (CMS 2012). Still, although the ACA provisions might increase access to mental health services that may be important for maintaining employment, private plans offered on the exchanges are not required to provide other employment-support services. Therefore, individuals with psychiatric disorders insured through them might still lack supports they need to obtain and maintain employment.
3. Coverage for Youths Up to Age 26
Under the ACA, young adults can remain enrolled in a parent's employer-based or individual insurance plan until they reach age 26 (ACA 2010). This provision is particularly important for TAY who experience their first mental health symptoms and may need EI to prevent psychosis. These young people often are not yet eligible for public health insurance coverage, as Medicaid coverage is generally unavailable for childless adults unless they meet the SSA definition of disability and have low earnings, making them eligible for SSI or SSDI benefits.26 Obtaining health care coverage through private plans is important for ensuring continued coverage of children with disabilities until age 26, and for ensuring that potentially disabling mental health symptoms are treated as they emerge.
4. Establishment of "Health Homes"
Under the Medicaid health home option established by the ACA, states are given an increased federal matching rate for reimbursing providers who offer "health home" services. The health home model--based on the medical home concept--is intended to enhance coordination of medical care, mental health, and substance use services, and community-based social services and supports for individuals with chronic illness (HHS 2010a). Health home services may be offered to individuals who: (1) have at least two chronic conditions; (2) have one chronic condition and are at risk for another; or (3) have one serious and persistent mental health condition. Services provided by a health home must include comprehensive care management, care coordination and health promotion, comprehensive transitional care from inpatient to other settings, individual and family support, referral to community and social support services when needed, and the use of health information technology when appropriate and feasible.
The health home option is designed to better integrate medical and behavioral health services, and is, therefore, highly relevant to individuals with mental health needs. A variety of health care providers can offer health home services, including community mental health centers or any other provider proposed by the state and approved by CMS (HHS 2010a). In their Medicaid State Plan amendments, states must describe the ways they will support health home providers in addressing a number of components, including coordinating and providing access to services for mental health and substance abuse, and providing referrals to community and social support services. Further, the ACA requires states to consult with SAMHSA regarding how best to address prevention and treatment of mental illness for individuals who are low income and/or who have one or more chronic illnesses. Although health homes are required to coordinate referrals of patients to social services--a broad category that could potentially include employment assistance--it is not clear whether those homes will necessarily provide employment services and supports. Also unclear is who will fund the social services or employment supports to which health home patients are referred.
5. Accountable Care Organizations
Accountable care organizations (ACOs) are provider-run entities in which the providers are responsible for the care of an entire enrolled population and may share in any cost savings that result from improvements in quality and efficiency of care (Gold et al. 2012). The ACA and subsequent regulations authorized the formation of ACOs within the Medicare program. However, a few states have started to independently plan and implement Medicaid ACO initiatives. Some states, including Oregon and Colorado, have begun plans to integrate behavioral health and medical care risk arrangements as part of their ACO initiatives. Theoretically, ACOs could provide employment supports to people with psychiatric disorders and other disabilities, but they are not required to do so.
6. Amendments to Medicaid Section 1915(i) HCBS State Plan Option
The ACA made a number of changes to the Section 1915(i) state option (see Chapter V for more details on 1915(i)) that may make it more relevant to states that wish to provide SE to Medicaid beneficiaries. Perhaps most importantly, amendments were made to expand the types of services that states can provide to Medicaid beneficiaries. The DRA authorized states to offer a variety of HCBS through 1915(i), including case management and home health aides, and, for individuals with mental illnesses, psychosocial rehabilitation services, clinic services, and day treatment and other partial-hospitalization services. However, the list of services that states could furnish was originally limited to those specifically mentioned in the statute. Revisions made by the ACA also allow "such other services requested by the State as the Secretary may approve" (HHS 2010b), which may include all aspects of SE (Siegwarth & Koyanagi 2012).
The ACA also expanded financial eligibility criteria for 1915(i) services. As originally enacted by the DRA, states could provide 1915(i) services only to those with incomes up to 150 percent of the FPL who were eligible for Medicaid in the state (HHS 2010b). These individuals did not have to qualify for an institutional level of care. In addition to preserving this eligibility group, the ACA expanded financial eligibility to include a new group of beneficiaries, described as follows in a CMS memo to State Medicaid Directors: "The ACA adds a new section to 1915(i) that allows States the option of providing services to individuals with income up to 300 percent of the SSI Federal benefit rate. While individuals served in this new eligibility group must be eligible for HCBS under a 1915(c), (d), or (e) waiver or 1115 demonstration program, they do not have to be enrolled and receiving services in either waiver program."27
Another alteration to the original DRA language made by the ACA prohibits state waiting lists. Under the DRA, states could limit the provision of 1915(i) services to individuals in certain areas of the state and were permitted to establish waiting lists. Under the ACA, states must provide services to all individuals who meet financial eligibility and the state's needs-based eligibility criteria (HHS 2010b). All services must now be offered statewide and cannot be limited to certain areas.
Finally, as originally authorized through the DRA, states were required to ensure comparability in 1915(i) services and, therefore, were not permitted to target programs to certain populations. Under the ACA, states are given new flexibility to offer services that vary by amount, duration, type, and scope to different population groups. Therefore, a state could now target a 1915(i) benefit specifically to persons with chronic mental illness for evidence-based SE services. As of February 2012, eight states had an approved 1915(i) state plan option28 (Bazelon Center 2012a; Siegwarth & Koyanagi 2012).
Some observers have speculated that several of the ACA's amendments to 1915(i) will deter widespread adoption (Justice 2011); states may be particularly reluctant to accept the prohibition of waiting lists, which eliminates their ability to control costs through enrollment caps. Nevertheless, states have great freedom in designing their needs-based criteria, which might serve as a lever for states to control eligibility and enrollment--and hence costs--by imposing stringent requirements. In addition, states may have a financial incentive to adopt the 1915(i) option in order to substitute federal Medicaid funds for the state and county funds that many currently use to provide services to adults with mental illness (Bazelon Center 2012). Furthermore, the ability to target particular populations provides new flexibility states can use to offer comprehensive SE services while containing the costs by limiting their availability to individuals with very serious mental health conditions. As of April 2014, 14 states had an approved 1915(i) state plan option or plan to implement one in 2014 (Kaiser Family Foundation 2013).
7. Other Aspects of the ACA That May Benefit Individuals with Psychiatric Disorders and Other Disabilities
Several other elements of the ACA have the potential to help those with psychiatric disorders and other disabilities to maintain employment. First, the law eliminates the ability of insurers to decline coverage for individuals with pre-existing conditions. Therefore, those who fall into this category will no longer have to leave the labor force to acquire coverage through Medicaid (Altarum Institute 2010a). Second, the law prohibits health plans from establishing annual and lifetime limits on the dollar value of EHB. Finally, employers can no longer use wage levels to determine who within the company will be eligible for health insurance. This means that individuals with psychiatric disorders and other disabilities who have lower-wage jobs should now have greater ability to gain insurance through their employers.
If the provision of employment-related services to those with psychiatric disorders and other disabilities results in successful employment, transitions between Medicaid and other subsidized insurance programs may be inevitable. If an individual's income rises above 138 percent of the FPL because of employment, the individual will no longer qualify for Medicaid and must transition to other subsidized health insurance coverage (Koyanagi et al. 2011). Such coverage transitions may seriously disrupt care due to several factors, including: (1) differences in mental health and employment support-related benefits available under Medicaid and plans available through the exchanges; (2) differences in pharmaceuticals covered under different plans; and (3) the possible need to change doctors, thereby compromising the therapeutic alliance. Further, individuals who do well in SE programs funded by Medicaid may lose access to those programs because of increased income. This could potentially result in an inability to maintain any progress they have made in their health and employment, possibly resulting in relapse, job loss, and a renewed need and eligibility for Medicaid services. The cycle of gaining and losing Medicaid benefits has been referred to as "churning." States that closely align their Medicaid and private insurance coverage options may ease care disruptions and ensure that individuals with mental illness and other disabilities have uninterrupted access to needed care.
The ACA's Medicaid expansion will broaden the population of individuals who are eligible for Medicaid to individuals without disabilities and to individuals with disabilities who do not meet SSA's criteria for disability benefits. States that expand Medicaid to cover newly eligible individuals with mental illnesses may have the opportunity to shift state mental health and CMHS Block Grant funds to finance other support services, such as SE. One analysis estimates that the Medicaid expansion could result in states replacing $11 billion to $22 billion of state mental health funding with Medicaid funds (Buttgens et al. 2011). Because more people with psychiatric disorders will have coverage through Medicaid and the exchanges, SAMHSA is strongly encouraging states to use CMHS Block Grant funds to support treatment and support services not funded by Medicaid and other payers after implementation of the ACA, and to fund prevention efforts (HHS 2012). This may reduce the disincentive for Social Security disability beneficiaries to keep earnings low to retain Medicaid coverage, since using this funding mechanism could make these services available to people who do not receive Medicaid.
C. Conclusion
The ACA contains many important provisions that will improve access to health insurance coverage and health care for individuals with disabilities, including those with SMI and other psychiatric disorders. Because some provisions have the potential to expand access to coverage, the ACA is a significant step toward breaking the link between eligibility for Social Security disability benefits and public health insurance. This step may weaken the incentive to forego employment and remain on Social Security disability benefits to retain health insurance coverage. Similarly, because the ACA extends medical coverage to those who heretofore have been ineligible for or unable to purchase coverage, it also has the potential to increase access to employment services and supports in a number of ways.
In January 2014, provisions of the ACA that allow states to expand their Medicaid programs went into effect. In states that accept this option, low-income and moderate-income residents who do not meet the definition of disability for SSI or SSDI or are otherwise ineligible for Medicaid will be able to obtain health insurance. As of January 2014, about half of the states are implementing this expansion. States have the flexibility to provide alternative benefits instead of traditional Medicaid services to individuals newly eligible for Medicaid under the ACA. On the other hand, they also have the option to provide the full package of Medicaid benefits to new beneficiaries and design benefit packages for specific populations, such as individuals with SMI. This option might encourage the expansion of Medicaid-funded employment supports. Additional Medicaid options, such as the option to offer health home services to certain Medicaid beneficiaries, the adoption of ACOs, and enhancements to the section 1915(i) state option for HCBS, might also serve as avenues for the provision of employment services. An individual's access to expanded Medicaid services, however, remains dependent upon the state in which he or she resides.
Other reforms to the private health insurance market are also likely to increase access to health insurance and services for people with mental illnesses. All new individual and small-group plans are required to offer mental health and substance use disorder services and comply with federal parity requirements. Prohibitions on pre-existing condition exclusions are also likely to offer individuals with pre-existing psychiatric disorders and other disabilities improved access to coverage, and restrictions on annual and lifetime limits are important for those with high health care costs. Though private plans are somewhat unlikely to cover a full range of employment services, increased availability of health insurance and consistent access to appropriate care are critical to a person's ability to maintain health and secure and retain employment.
VII. Conclusion
Our literature review found that evidence-based SE provides the strongest evidence for helping people with SMI to find work, but there is little strong evidence for positive long-term outcomes. The absence of improved long-term outcomes may result from work disincentives built into Social Security disability and Medicaid programs that discourage more than minimal levels of work, or from lack of long-term funding options for SE. The ACA may provide a better source of long-term funding, since it expands the population of individuals eligible for Medicaid and offers additional options for health insurance coverage.
The ACA may support workers with mental health impairments by expanding availability of vocational and other support services along with health insurance among new SSDI beneficiaries with mental health impairments, leading to improved short-term employment outcomes for this group and perhaps fewer applications among individuals considering applying for SSDI. The ACA may also support workers by expanding eligibility for health insurance among low-wage workers who experience SMI and among individuals who experience a psychiatric disorder that does not qualify them for Social Security disability benefits.
Evidence suggests that intervening early may help prevent full-blown psychosis and long-term involvement with the mental health and disability systems, especially when the intervention includes an SE component. Because the ACA enables youth to remain on their parents' insurance until age 26, mental health services and maybe even SE may become more available to this population. Our analysis shows a consistent decline in employment as early as three years before SSDI receipt. Targeting individuals who leave employment due to a mental illness and go on to apply for means-tested benefits or private disability insurance, or those with high health expenditures or those receiving workers' compensation benefits may reduce future applications for SSDI.
References
Adler, D., T. McLaughlin, W. Rogers, H. Chang, L. Lapitsky, & D. Lerner. "Job Deficits Due to Depression." American Journal of Psychiatry, 2006, pp.1569-1576.
Altarum Institute. "Analysis of Affordable Care Act in Relation to the Employment of Persons with Disabilities."Ann Arbor, MI: Altarum Institute, 2010a.
Altarum Institute. "An Independent Evaluation of the Community Mental Health Services Block Grant." Report #10-4610a, Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, 2010b.
Altshuler, N., S. Prenovitz, B. O'Day, & G. Livermore. "Provider Experiences Under the Revised Ticket to Work Regulations: Final report." Washington, DC: Center for Studying Disability Policy, Mathematica Policy Research, 2011.
Anthony, W. "Supported Employment." The National Gains Center for Systemic Change for Justice-Involved People with Mental Illness, May 2006. Available at http://gainscenter.samhsa.gov/pdfs/ebp/Supported_Employment.pdf. Accessed 2/1/13.
Beronio, K., R. Po, L. Skopec, & S. Glied. "Affordable Care Act Expands Mental Health and Substance Use Disorder Benefits and Federal Parity Protections for 62 Million Americans." ASPE Research Brief. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, February 2013.
Bird, V. "Early Intervention Services, Cognitive Behavioral Therapy, and Family Intervention in Early Psychosis: Systematic Review." British Journal of Psychiatry, 2010, 197(5), pp. 350-356.
Binder, C. "Medicaid Targeted Case Management (TCM) Benefits."Report #RL34426. Washington, DC: Congressional Research Service, 2008.
Blyler, C.R. "Understanding the Employment Rate of People with Schizophrenia: Different Approaches Lead to Different Implications for Policy." In Principles of Experimental Psychopathology: Essays in Honor of Brendan A. Maher, M.F. Lenzenweger & J.M. Hooley (editors). Washington, DC: American Psychological Association, 2003.
Bohman, T.M., L. Wallisch, K. Christensen, D. Stoner, A. Pittman, B. Reed, et al. "Working Well-the Texas Demonstration to Maintain Independence and Employment: 18-month Outcomes." Journal of Vocational Rehabilitation, 2011, pp. 97-106.
Bond, G.R. "Supported Employment: Evidence for an Evidence-Based Practice." Psychiatric Rehabilitation Journal, Spring 2004, 27(4), pp. 345-359.
Bond, G.R., D.R. Becker, R.E. Drake, C.A. Rapp, N. Meisler, A.F. Lehman, M.D. Bell, & C.R. Blyler. "Implementing Supported Employment as an Evidence-Based Practice." Psychiatric Services, March 2001, 52(3), pp. 313-322.
Bond, G.R., L.L. Dietzen, J.H. McGrew, & L.D. Miller."Accelerating Entry Into Supported Employment for Persons with Severe Psychiatric Disabilities." Rehabilitation Psychology, Summer 1995, 40(2), pp.75-94.
Bond, G.R., M.P. Salyers, J. Dincin, R.E. Drake, D.R. Becker, V.V. Fraser, & M. Haines. "A Randomized Controlled Trial Comparing Two Vocational Models for Persons with Severe Mental Illness." Journal of Consulting and Clinical Psychology, December 2007, 75(6), pp. 968-982.
Bond, G., R. Drake, K. Mueser, & E. Latimer. "Assertive Community Treatment for People with Severe Mental Illness: Critical Ingredients and Impact on Patients." Disease Management and Health Outcomes, 2001, 9(3), pp. 141-159.
Bond, G.R., R.E. Drake, & D.R. Becker. "An Update on Randomized Controlled Trials." Psychiatric Rehabilitation Journal, 2008, 31(4), pp. 280-290.
Browne, D.J., & G. Waghorn. "Employment Services as an Early Intervention for Young People with Mental Illness." Early Intervention in Psychiatry, November 2010, 4(4), pp. 327-335.
Burke-Miller, J., L.A. Rassano, D.D. Grey, C.R. Blyler, & J.A. Cook."Supported Employment Outcomes for Transition Age Youth and Young Adults." Psychiatric Rehabilitation Journal, Winter 2012, 35(3), pp. 171-179.
Burns, T., J. Catty, T. Becker, R.E. Drake, A. Fioritti, et al. "The Effectiveness of Supported Employment for People with Severe Mental Illness: A Randomised Controlled Trial." Lancet, September 2007, 370(9593), pp. 1146-1152.
Burt, M.R. "Impact of Housing and Work Supports on Outcomes for Chronically Homeless Adults with Mental Illness: LA's HOPE." Psychiatric Services, 63(3), pp. 209-215.
Burton, W.N., C.-Y. Chen, D.J. Conti, A.B. Schultz, & D.W. Edington. "The Association of Antidepressant Medication Adherence With Employee Disability Absences." American Journal of Managed Care, 2007, pp. 105-112.
Buttgens, M., S. Dorn, & C. Carroll. "Consider Savings as well as Costs: State Governments Would Spend at Least $90 Billion Less With the ACA than Without It from 2012 to 2019." Washington, DC: Urban Institute, 2011. Available at http://www.urban.org/uploadedpdf/412361-consider-savings.pdf/.
Campbell, K., G.R. Bond, & R.E. Drake. "Who Benefits from Supported Employment: A Meta-Analytic Study." Schizophrenia Bulletin, 2009, 37(2), pp. 370-380.
Carroll, C., J. Rick, H. Pilgrim, J. Cameron, & J. Hillage."Workplace Involvement Improves Return to Work Rates Among Employees with Back Pain on Long-Term Sick Leave: A Systematic Review of the Effectiveness and Cost-Effectiveness of Interventions." Disability & Rehabilitation, 2010, 32(8), pp. 607-621.
Cavenaugh, B., & J.M. Giesen. "A Systematic Review of Transition Interventions Affecting the Employability of Youths with Visual Impairments." Journal of Visual Impairment & Blindness, 2012, 106(7), pp. 400-413.
Coe, N.B., & M.S. Rutledge. "How Does the Composition of Disability Insurance Applicants Change Across Business Cycles?" Working Paper #2013-5. Chestnut Hill, MA: Center for Retirement Research at Boston College, 2013.
Centers for Medicare and Medicaid Services, Center for Consumer Information and Insurance Oversight, "Essential Health Benefits Bulletin," December 2011. Available at http://cciio.cms.gov/resources/files/Files2/12162011/essential_health_benefits_bulletin.pdf.
Centers for Medicare and Medicaid Services. "2011 CMS Statistics." Available at https://www.cms.gov/ResearchGenInfo/02_CMSStatistics.asp#TopOfPage. Accessed May 23, 2012.
Centers for Medicare and Medicaid Services. "Letter to State Medicaid Directors from the CMS Deputy Administrator/Director of the Center for Medicaid and CHIP Services regarding Essential Health Benefits in the Medicaid program." Baltimore, MD: Centers for Medicare and Medicaid Services, November 20, 2011.
Chandler, D., J. Meisel, T. Hu, M. McGowen, & K. Madison. "Client Outcomes in a Three-Year Controlled Study of an Integrated Service Agency Model." Psychiatric Services, December 1996, 47(12), pp. 1337-1343.
Chow, C.M. "Reasonable Job Accommodations: An Econometric Investigation into Strategies Addressing Barriers to Employment for Individuals with Psychiatric Disabilities." Waltham, MA: August 2012.
Cimera, R.E. "The Economics of Supported Employment: What New Data Tell Us." Journal of Vocational Rehabilitation, 2012, 37(2), pp. 109-117.
Clayton, S., C. Bambra, R. Gosling, S. Povall, K. Misso, & M. Whitehead. "Assembling the Evidence Jigsaw: Insights from a Systematic Review of UK Studies of Individual Focused Return to Work Initiatives for Disabled and Long-Term Ill People." BMC Public Health, 2011, 11(1), pp. 170-181.
Congressional Budget Office. "Estimates for the Insurance Coverage Provisions of the Affordable Care Act Updated for the Recent Supreme Court Decision." Washington, DC: Congressional Budget Office, 2012. Available at http://www.cbo.gov/publication/43472.
Connecticut Department of Mental Health and Addiction Services."Mental Health Waiver: Working for Integration Support and Empowerment (WISE)." Available at http://www.ct.gov/dmhas/cwp/view.asp?a=2902&q=423430. Accessed December 31, 2012.
Connecticut Department of Mental Health and Addiction Services. "Mental Health Waiver Program Participant Eligibility Requirements."Available at http://www.ct.gov/dmhas/lib/dmhas/oaswise/eligibilityrequirements.pdf. Accessed December 31, 2012.
Cook, J.A., C.R. Blyler, H.S. Leff, W.R. McFarlane, R.W. Goldberg, et al. "The Employment Intervention Demonstration Program: Major Findings and Policy Implications." Psychiatric Rehabilitation Journal, Spring 2008, 31(4), pp. 291-295.
Cook, J.A., & J. Burke. "Public Policy and Employment of People with Disabilities: Exploring New Paradigms." Journal of Behavioral Science & the Law, 2002, 20, pp. 541-557.
Cook, J., J. Burke-Miller, J, Jonikas, & M. Swarbrick. "Asset Development for People with Psychiatric Disabilities: The Essential Role of Financial Security in Recovery." 2010. Available at http://www.cmhsrp.uic.edu/download/NRTC4.IDA%20Project%20Report.10.25.10.pdf.
Cook, J.A., H.S. Leff, C.R. Blyler, P.B. Gold, R.W. Goldberg, R.E. Clark, et al. "Estimated Payments to Employment Service Providers for Persons with Mental Illness in the Ticket to Work Program," Psychiatric Services, 2006, 57(4), pp. 465-471.
Cook, J.A., S. Leff, C.R. Blyler, P.B. Gold, R.W. Goldberg, K.T. Mueser, M.G. Toprac, W.R. McFarlane, M.S. Shafer, L.E. Blankertz, K. Dudek, L.A. Razzano, D.D. Grey, & J. Burke-Miller. "Results of a Multisite Randomized Trial of Supported Employment Interventions for Individuals with Severe Mental Illness." Archives of General Psychiatry, May 2005, 62(5), pp. 505-512.
Cook, J.A., A.F. Lehman, R.E. Drake, W.R. McFarlane, P.B. Gold, H.S. Leff, et al. "Integration of Psychiatric and Vocational Services: A Multi-site Randomized, Controlled Trial of Supported Employment." American Journal of Psychiatry, 2005a, 162(10), pp. 1948-1956.
Cook, J., C. Russell, D. Grey, & J. Jonikas. "A Self-Directed Care Model for Mental Health Recovery." Psychiatric Services, 2008, 59(6), pp. 600-602
Daly, M.C. "Characteristics of SSI and DI Recipients in the Years before Receiving Benefits." In Growth in Disability Benefits, K. Rupp and D.C. Stapleton (editors). Kalamazoo, MI: W.E. Upjohn Institute for Employment Research, 1998.
Dartmouth IPS Supported Employment Center. "Johnson & Johnson--Dartmouth Community Mental Health Program."Available at http://www.dartmouth.edu/~ips/page3/page10/page10.html. Accessed January 6, 2013.
Davis, L.L., A.C. Leon, R. Toscano, C.E. Drebing, L.C. Ward, P.E. Parker, T.M. Kashner, & R.E. Drake. "A Randomized Controlled Trial of Supported Employment among Veterans with Posttraumatic Stress Disorder." Psychiatric Services, 2012, 63(5), pp. 464-470.
Dewa, C.S., J.S. Hoch, E. Lin, M. Paterson, & P. Goering. "Pattern of Antidepressant Use and Duration of Depression-Related Absence from Work." British Journal of Psychiatry, 2003, pp. 507-513.
Dibben, P., G. Wood, R. Nicolson, & R. O'Hara. "Quantifying the Effectiveness of Interventions for People with Common Health Conditions in Enabling Them to Stay in or Return to Work: A Rapid Evidence Assessment." Research Report #812. Department for Work and Pensions, 2012.
Doughty, C., & T. Sampson. "The Effectiveness of Service User-run or Service User-led Mental Health Services for People with Mental Illness: A Systematic Literature Review". A Mental Health Commission Report; Mental Health Commission, Wellington, New Zealand, 2005.
Drake, R.E., D.R. Becker, H.H. Goldman, & R.A. Martinez."The Johnson & Johnson--Dartmouth Community Mental Health Program: Disseminating Evidence-Based Practice." Psychiatric Services, March 2006, 57(3), pp. 302-304.
Drake, R.E., G.J. McHugo, D.R. Becker, W.A. Anthony, & R.E. Clark. "The New Hampshire Study of Supported Employment for People With Severe Mental Illness." Journal of Consulting & Clinical Psychology, April 1996, 64(2), pp. 391-399.
Drake, R.E., G.J. McHugo, R.R. Bebout, D.R. Becker, M. Harris, G.R. Bond, & E. Quimby. "A Randomized Clinical Trial of Supported Employment for Inner-city Patients WithSevere Mental Disorders." Archives of General Psychiatry, 1999, 56(7), pp. 627-633.
Fields, S. "Leveraging Medicaid for Supported Employment: Options for states" Philadelphia, PA: Westat, n.d. Available at http://www.nasuad.org/documentation/hcbs2010/PowerPoints/Sunday/Blending%20and%20Braiding%20Medicaid%20and%20Other%20Financing.pdf.
Fossey, E.M., & C.A. Harvey. "Finding and Sustaining Employment: A Qualitative Meta-synthesis of Mental Health Consumer Views." Canadian Journal of Occupational Therapy, 2010, pp. 303-314.
Fowler, D., J. Hodgekins, L. Howells, M. Millward, A. Ivins, & G. Taylor. "Can Targeted Early Intervention Improve Functional Recovery in Psychosis? A Historical Control Evaluation of the Effectiveness of Different Models of Early Intervention Service Provision in Norfolk 1998-2007." Early Intervention in Psychiatry, November 2009, 3(4), pp. 282-288.
Fraker, T. "The Youth Transition Demonstration: Lifting Employment Barriers for Youth with Disabilities." Report #13-01. Washington, DC: Center for Studying Disability Policy, February 2013.
Fraker, T. "The Youth Transition Demonstration: Interim Findings and Lessons for Program Implementation." Report #11-04. Washington, DC: Center for Studying Disability Policy, October 2011.
Frey, W., R.E. Drake, G. Bond, A.L. Miller, H.H. Goldman, D.S. Salkever, S. Holsenbeck, M. Karakus, R. Milfort, J. Riley, C. Reidy, J. Bollmer, & M. Collins. "Mental Health Treatment Study Final Report." Rockville, MD: July, 2011.
Furlan, A., W. Gnam, N. Carnide, E. Irvin, B. Amick III, K. DeRango, et al. "Systematic Review of Intervention Practices for Depression in the Workplace." Toronto: Institute for Work and Health, 2011.
Gao, N., W.R. Waynor, & S. O'Donnell. "Creating Organizational Commitment to Change: Key to Consumer Employment Success in a Supportive Housing Agency." Journal of Vocational Rehabilitation, 2009, 31(1), pp. 45-50.
Garety, P.A., T.K.J. Craig, G. Dunn, M. Fornells-Ambrojo, S. Colbert, N. Rahaman, J. Reed, & P. Power. "Specialised Care for Early Psychosis: Symptoms, Social Functioning, and Patient Satisfaction." British Journal of Psychiatry, January 2006, 188(1), pp. 37-45.
Garfield, R.L., S.H. Zuvekas, J.R. Lave, & J.M. Donohue."The Impact of National Health Care Reform on Adults with Severe Mental Disorders." American Journal of Psychiatry, 2011, 168(5), pp. 486-494.
Goertz, Y., B. van Lierop, I. Houkes, & F. Nijhuis."Factors Related to the Employment of Visually Impaired Persons: A Systematic Literature Review." Journal of Visual Impairment & Blindness, 2010, 104(7), pp. 404-418.
Gold, M., J. Nysenbaum, & S. Streeter. "Emerging Medicaid Accountable Care Organizations: The Role of Managed Care." Report #8319. Washington, DC: Kaiser Commission on Medicaid and the Uninsured, 2012.
Gold, P.B., N. Meisler, A.B Santos, M.A Carnemolla, O.H Williams, & J. Keleher. "Randomized Trial of Supported Employment Integrated with Assertive Community Treatment for Rural Adults with Severe Mental Illness." Schizophrenia Bulletin, 2006, 32(2), pp. 378-395.
Goldstrom, I.D., J. Campbell, J.A. Rogers, D.B. Lambert, B. Blacklow, M.J. Henderson, & R.W. Manderscheid "National Estimates for Mental Health Mutual Support Groups, Self-Help Organizations, and Consumer-Operated Services." Administration and Policy in Mental Health and Mental Health Services Research, 33(1), pp. 92-103.
Gensby, U., A-M. Klint Jørgensen, T. Filges, K. Kowalski, M. Labriola, T. Lund, B.C. Amick III, & M. Saidj. "Workplace Disability Management Programs Promoting Return to Work: A Systematic Review". Campbell Systemic Reviews. 2012.
Haber, M.G., A. Karpur, N. Deschênes, & H.B. Clark. "Predicting Improvement of Transitioning Youth People in the Parternships for Youth Transition Initiative: Findings from a Multisite Demonstration." Journal of Behavioral Health Services & Research, October 2008, 35(4) Special Issue, pp. 488-512.
Harpaz-Rotem, I., R.A. Rosenheck, & R. Desai. "Residential Treatment for Homeless Female Veterans with Psychiatric and Substance Use Disorders: Effect on 1-Year Clinical Outcomes." Journal of Rehabilitation Research & Development, 2011, 48(8), pp. 891-899.
Heidkamp, M., & W. Mabe. "The Great Recession and Serving Dislocated Workers with Disabilities: Perspectives from One-Stop Career Centers and Rapid Response Coordinators." Rutgers, NJ: National Technical Assistance and Research Center to Promote Leadership for Increasing the Employment and Economic Independence of Adults with Disabilities; U.S. Department of Labor, Office of Disability Employment Policy, 2011.
Henry, L.P., P. Amminger, M.G. Harris, H.P. Yuen, S.M. Harrigan, et al. "The EPPIC Follow-Up Study of First-Episode Psychosis: Longer-Term Clinical and Functional Outcome 7 Years AfterIndex Admission." Journal of Clinical Psychiatry, June 2010, 71(6), pp. 716-728.
Honeycutt, T.. "Program and Benefit Paths to the Social Security Disability Insurance Program." Journal of Vocational Rehabilitation, 2004, 21(2), pp. 83-94.
Hutchinson, D., W. Anthony, L. Ashcraft, E. Johnson, E. Dunn, A. Lyass, & S. Rogers. "The Personal and Vocational Impact of Training and Employing People with Psychiatric Disabilities as Providers."Psychiatric Rehabilitation Journal, 2006, 29(3), pp. 205-213.
Insel, T., "Assessing the Economic Costs of Serious Mental Illness," American Journal of Psychiatry, June 2008, 165(6), pp. 663-665.
Johnson, K., P. Brown, M. Harniss, & K. Schomer. "Knowledge Translation in Rehabilitation Counseling." Rehabilitation Education, 2010, 24(3&4), pp. 239-250.
Judge David L. Bazelon Center for Mental Health Law. "Supported Employment Fact Sheet." Washington, DC: Judge David L. Bazelon Center for Mental Health Law, 2010. Available at http://www.bazelon.org/LinkClick.aspx?fileticket=IVd2OXBERnI%3d&tabid=350.
Judge David L. Bazelon Center for Mental Health Law. "The Affordable Care Act at Year Two." Washington, DC: Judge David L. Bazelon Center for Mental Health Law, 2012a. Available at http://www.bazelon.org/LinkClick.aspx?fileticket=vluo7GUqOaA%3d&tabid=77.
Judge David L. Bazelon Center for Mental Health Law. "Take Advantage of New Opportunities to Expand Medicaid Under the Affordable Care Act." Washington, DC: Judge David L. Bazelon Center for Mental Health Law, 2012b. Available at http://www.bazelon.org.
Justice, D. "Implementing the Affordable Care Act: New Options for Medicaid Home and Community Based Services." Briefing. Portland, ME: National Academy for State Health Policy, October 2011.
Kaiser Family Foundation. "Explaining Health Care Reform: Questions about Health Insurance Subsidies." Report #7692-02. Washington, DC: Kaiser Family Foundation, 2012.
Kaiser Family Foundation. "Implementing New Private Health Insurance Market Rules." Report #8399. Washington, DC: Kaiser Family Foundation, 2013.
Karakus, M., W. Frey, H. Goldman, S. Fields, & R. Drake. "Federal Financing of Supported Employment and Customized Employment for People with Mental Illnesses: Final Report." U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy, 2011. Available at http://aspe.hhs.gov/daltcp/reports/2011/supempFR.htm.
Karpur, A., H.B. Clark, P. Caproni, & H. Sterner. "Transition to Adult Roles for Students with Emotional/Behavioral Disturbances: A Follow-Up Study of Student Exiters From Steps-to-Success." Career Development for Exceptional Individuals, Spring 2005, 28(1), pp. 36-46.
Khan, F., & T. Stokes. "Effectiveness of Vocational Rehabilitation Intervention on the Return to Work and Employment of Persons with Multiple Sclerosis." Cochrane Database of Systematic Reviews, 2011, 12.
Killackey, E., H.J. Jackson, & P.D. McGorry. "Vocational Intervention in First-Episode Psychosis: Individual Placement and Support v. Treatment as Usual."British Journal of Psychiatry, August 2008, 193(2), pp. 114-120.
Koyanagi, C., R.L. Garfield, J. Howard, & B. Lyons. "Medicaid Policy Options for Meeting the Needs of Adults with Mental Illness Underthe Affordable Care Act." Report #8181. Washington, DC: Kaiser Commission on Medicaid and the Uninsured, 2011. Available at http://www.kff.org.
Koyanagi, C., R. Summers, & J. Yedziniak. "Adding Support Services to Medicaid: Now You Can." Washington, DC: Judge David L. Bazelon Center for Mental Health Law, 2010. Available at http://www.bazelon.org.
Krupa, T. "Interventions to Improve Employment Outcomes for Workers Who Experience Mental Illness." Canadian Journal of Psychiatry, 2007, pp. 339-345.
Lanctot, N., M. Corbiere, & M-J. Durand. "Job Tenure and Quality of Work Life of People with Psychiatric Disabilities Working in Social Enterprises."Journal of Vocational Rehabilitation, 2012, 37, pp. 39-48.
Latimer, E.A., T. Lecomte, D.R. Becker, R.E. Drake, I. Duclos, M. Piat, & N. Lahaie. "Generalisability of the Individual Placement and Support Model of Supported Employment: Results of a Canadian Randomised Controlled Trial." British Journal of Psychiatry, 2006, 189(191) , pp. 65-73.
Lauber, C., & J.L. Bowen. "Low Mood and Employment: When Affective Disorders are Intertwined with the Workplace--A UK Perspective."International Review of Psychiatry, 2010, pp. 173-182.
Lehman, A.F., R. Goldberg, L.B. Dixon, S. McNary, L. Postrado, A. Hackman, & K. McDonnell. "Improving Employment Outcomes for Persons with Severe Mental Illness." Archives of General Psychiatry, February 2002, 59(2), pp. 165-172.
Levy, A., B. Bruen, & L. Ku, "The Potential Employment Impacts of Health Reform on Working-Age Adults with Disabilities." Journal of Disability Policy Studies, online May 30, 2012. (DOI: 10.1177/1044207312446225).
Linkins, K.W., J.J. Brya, A. Oelschlaeger, B. Simonson, S. Lahiri, J. McFeeters, M. Schutze, J. Jonas, & M.A. Mowry. "Influencing the Disability Trajectory for Workers with Serious Mental Illness: Lessons from Minnesota's Demonstration to Maintain Independence and Employment." Journal of Vocational Rehabilitation, 2011, 34(2), pp. 107-118.
Lindner, S.. "From Working to Applying: Employment Transitions of Applicants for Disability Insurance in the United States." Journal of Social Policy, 2013, 42(2), pp 329-348.
Lindner, S., & A. Nichols. "The Impact of Temporary Assistance Programs on Disability Rolls and Re-Employment." Working Paper #2012-2. Chestnut Hill, MA: Center for Retirement Research at Boston College, 2012.
Livermore, G.A., & N. Goodman. "A Review of Recent Evaluation Efforts Associated with Programs and Policies Designed to Promote the Employment of Adults with Disabilities." Washington, DC: Mathematica Policy Research, Rehabilitation Research and Training Center on Employment Policy for Persons with Disabilities, February 2009.
Livermore, G., D. Stapleton, & H. Claypool. "Health Care When Workers Need It Most: Before and After Entry into the Social Security Insurance Program." Inquiry, 2010, 47, pp. 135-149.
Livermore, G., A. Mamun, J. Schimmel, & S. Prenovitz. "Executive Summary of the Seventh Ticket to Work Evaluation Report." Washington, DC: Mathematica Policy Research, 2013.
Lounds Taylor, J., M.L. McPheeters, N.A. Sathe, D. Dove, Je. Veenstra-VanderWeele, & Z. Warren. "A Systematic Review of Vocational Interventions for Young Adults with Autism Spectrum Disorders." Pediatrics, 2012, 130(3), pp. 531-538.
Macias, C., C.F. Rodican, W.A. Hargreaves, D.R. Jones, P.J. Barreira, & Q. Wang. "Supported Employment Outcomes of a Randomized Controlled Trial of ACT and Clubhouse Models." Psychiatric Services, October 2006, 57(10), pp. 1406-1415.
Maestas N. "Securing the Future of the Social Security Disability Insurance Program." Testimony presented before the House Committee on Ways and Means, Subcommittee on Social Security, March 20, 2012. Available at http://www.rand.org/content/dam/rand/pubs/testimonies/2012/RAND_CT373.pdf.
Major, B.S., M.F. Hinton, A. Flint, A. Chalmers-Brown, K. McLoughlin, & S. Johnson. "Evidence of the Effectiveness of a Specialist Vocational Intervention Following First Episode Psychosis: A Naturalistic Prospective Cohort Study." Social Psychiatry & Psychiatric Epidemiology, January 2010, 45(1), pp. 1-8.
Marrone, J. "Creating Hope ThroughEmployment for People Who are Homeless or in Transitional Housing". American Journal of Psychiatric Rehabilitation, 2005, 8(1), pp. 13-35.
Martin, F., A. Collins, & B. O'Day. "A Review of Systematic Reviews of Return-to-Work and Employment Support Interventions for People with Physical, Developmental Intellectual Disabilities." Task 9 Literature Review for U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Washington DC: Mathematica Policy Research, April 2013.
McDermid, L., S. Durie, J. McLean, & A. Woodhouse. "Making an Impact: Exploring How to Measure the Mental Health Impacts of Working in a Social Firm." Social Firms Scotland and Scottish Development Center for Mental Health, 2008.
McFarlane, W.R., R.A. Dushay, S.M. Deakins, P. Stastny, E.P. Lukens, J. Toran, & B. Link. "Employment Outcomes in Family-Aided Assertive Community Treatment." American Journal of Orthopsychiatry, April 2000, 70(2), pp. 203-214.
McFarlane, W.R., W.L. Cook, D. Downing, A. Ruff, S. Lynch, et al. "Early Detection, Intervention, and Prevention of Psychosis Program: Rationale, Design, and Sample Description." Adolescent Psychiatry, April 2012, 2(2), pp. 112-124.
McFarlane, A.R.Y., P.D. Mcgorry, H.J. Jackson, G.C. Patton, & A. Rakkar. "Monitoring and Care of Young People at Incipient Risk of Psychosis" Schizophrenia Bulletin, 1996, 22(2), pp. 283-303.
McKeown K., T. O'Brien, & G. Fitzgerald. "Vocational Rehabilitation and Mental Health: The European Project on Mental Health in Ireland 1989-1991." Evaluation Report Summary #1. Azimuth: 1992.
McNabb, J., D. Timmons, J. Song, & C. Puckett. "Uses of Administrative Data at the Social Security Administration." Social Security Bulletin, 2009, 69(1), pp. 75-84.
Michalopoulos, C., D. Wittenburg, D. Israel, J. Schore, A. Warren, A. Zutshi, S. Freedman, & L. Schwartz. "The Accelerated Benefits Demonstration and Evaluation Project: Impacts on Health and Employment at Twelve Months." MDRC report for the Social Security Administration, 2011. Available at http://www.mdrc.org/sites/default/files/private/full_528.pdf. Accessed February 1, 2013.
Mowbray, C., M. Collins, C. Bellamy, D. Megivern, D. Bybee, and S. Szilvagyi. "Supported Education for Adults with Psychiatric Disabilities: An Innovation for Social Work and Psychosocial Rehabilitation Practice." Social Work, 2005, 50(1), pp. 7-20.
Mueser, K.T., R.E. Clark, M. Haines, R.E. Drake, G.J. McHugo, G.R. Bond, S.M. Essock, D.R. Becker, R. Wolfe, & K. Swain. "The Hartford Study of Supported Employment for Persons with Severe Mental Illness." Journal of Consulting & Clinical Psychology, June 2004, 72(3), pp. 479-490.
Musumeci, M. "A Guide to the Supreme Court's Affordable Care Act Decision." Report #8332. Washington, DC: Kaiser Family Foundation, 2012. Available at http://www.nashp.org/sites/default/files/private/LTSS_SCAN-FINAL-9-29-10.PDF.
Nieuwenhuijsen, K., U. Bültmann, A. Neumeyer-Gromen, A.C. Verhoeven, J.H. Verbeek, & C.M. Feltz-Cornelis. "Interventions to Improve Cccupational Health in Depressed People."Cochrane Database of Systematic Reviews, November 1, 2008.
Nuechterlein, K. "Maximizing Successful Return to School or Work after an Initial Episode of Schizophrenia." Schizophrenia Research, 2012, 136(supplement 1), pp. 5-14.
Nuechterlein, K.H., K.L. Subotnik, L.R. Turner, & J. Ventura."Individual Placement and Support for Individuals with Recent-Onset Schizophrenia: Integrating Supported Education and Supported Employment." Psychiatric Rehabilitation Journal, Spring 2008a, 31(4), pp. 340-349.
Nuechterlein, K., K. Subotnik, J. Ventura, M. Gitlin, D. Gretchen-Doorly, et al. "A Randomized Controlled Trial of Supported Employment and Education and Workplace Skills Training in Recent-Onset Schizophrenia: Notable Improvements in Recovery." Schizophrenia Research, June 2008b, 102(1, supplement 2), p. 28.
O'Day, B., C. Blyler, R. Kleinman, B. Fischer, E. Morris, & L. Shottenfeld. "Improving Employment Outcomes for People with Psychiatric Disabilities." Task 3 Literature Review and Report for U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Washington, DC: Mathematica Policy Research, February 2013.
O'Malley Watts, M. "Money Follows the Person: A 2011 Survey of Transitions, Services, and Costs." Report #8142-02. Washington, DC: Kaiser Commission on Medicaid and the Uninsured, 2011. Available at http://www.kff.org.
Osher, F.C., & H.J. Steadman. "Adapting Evidence-Based Practices for Persons with Mental Illness Involved with the Criminal Justice System." Psychiatric Services, 2007, 58(11), pp. 1472-1478.
Osher, F., D.A. D'Amora, M. Plotkin, N. Jarrett, & A. Eggleston."Adults with Behavioral Health Needs under Correctional Supervision: A Shared Framework for Reducing Recidivism and Promoting Recovery." New York, NY: Council of State Governments, Justice Center, 2012.
Ownsworth, T., & K. McKenna. "Investigation of Factors Related to Employment Outcome Following Traumatic Brain Injury: A Critical Review and Conceptual Model." Disability & Rehabilitation, 2004, 26(13), pp. 765-784.
Patient Protection and Affordable Care Act, 42 U.S.C. § 2714 (2010).
Porteous, N., & G. Waghorn. "Implementing Evidence-Based Supported Employment Services in New Zealand for Young Adults with Psychosis: Progress During the First Five Years." British Journal of Occupational Therapy, December 2007, 70(12), pp. 521-526.
Prewitt, E., D. Stoner, L. Reagan, J. Buchenauer, & R. Hendler "Opportunities for States to Serve Individuals with Mental Illness through Money Follows the Person National Association of State Mental Health Program Directors." 2011. Available at http://www.nasmhpd.org/Meetings/webinars_MFP.aspx.
Pruett, S.R., E.A. Swett, F. Chan, D.A. Rosenthal, & G.K. Lee. "Empirical Evidence Supporting the Effectiveness of Vocational Rehabilitation." Journal of Rehabilitation, 2008, 74(2), pp. 56-63.
RAISE Early Treatment Program. "Overview of Project." Available at http://www.raiseetp.org/. Accessed January 3, 2013.
Resnick, S., & R. Rosenheck. "Dissemination of Supported Employment in Department of Veterans Affairs." Journal of Rehabilitation Research & Development, 2007, 44(6), pp. 867-878.
Revell, G., F. Smith, & K. Inge "An Analysis of Self-Employment Outcomes within the Federal/State Vocational Rehabilitation System." Journal of Vocational Rehabilitation, 2009, 31, pp. 11-18.
Rinaldi, M., R. Perkins, K. McNeil, N. Hickman, & S.P. Singh. "The Individual Placement and Support Approach to Vocational Rehabilitation for Young People with First Episode Psychosis in the UK." Journal of Mental Health, December 2010, 19(6), pp. 483-491.
Rogers, E.S., G.B. Teague, C. Lichtenstein, J. Campbell, A. Lyass, R. Chen, & S. Banks. "Effects of Participation in Consumer-Operated Service Programs on Both Personal and Organizationally Mediated Empowerment: Results of a Multisite Study." Journal of Rehabilitation Research & Development, 2007, 44(6), pp. 785-800.
Rosenbaum, S., J. Teitelbaum, & K. Hayes, "The Essential Health Benefits Provisions of the Affordable Care Act: Implications for People with Disabilities." The Commonwealth Fund, March 2011, 3.Available at http://www.commonwealthfund.org/~/media/Files/Publications/Issue%20Brief/2011/Mar/1485_Rosenbaum_essential_hlt_benefits_provisions_ACA_disabilities_reform_brief_v2.pdf.
Rosenheck, R.A., & A.S. Mares. "Implementation of Supported Employment for Homeless Veterans with Psychiatric or Addiction Disorders: Two-Year Outcomes." Psychiatric Services, 2007, 58(3), pp. 325-333.
Sarata, A.K. "Mental Health Parity and the Patient Protection and Affordable Care Act of 2010." Report #7-5700. Washington, DC: Congressional Research Service, 2011.
Saunders, J.L., M.J. Leahy, C. McGlynn, & N. Estrada-Hernandez."Predictors of Employment Outcomes for Persons with Disabilities: An Integrative Review of Potential Evidenced-Based Factors." Journal of Applied Rehabilitation Counseling, 2006, 37(2), pp. 3-20.
Schandelmaier, S., S. Ebrahim, S.C.A. Burkhardt, W.E.L de Boer, T. Zumbrunn, G.H. Guyatt, J.W. Busse, & R. Kunz. "Return to Work Coordination Programmes for Work Disability: A Meta-Analysis of Randomised Controlled Trials." PLoS ONE, 2012, 7(11), pp. e49760.
Schleiter, M.K., A. Statham, & T. Reinders. "Challenges Faced by Women with Disabilities under TANF." Journal of Women, Politics & Policy, 27(3-4), pp. 81-95.
Schmidt, L., K. Gill, C. Pratt, & P. Solomon. "Comparison of Service Outcomes of Case Management Teams with and without a Consumer Provider."American Journal of Psychiatric Rehabilitation, vol 11, pp. 310-329.
Schnittker, J., M. Massoglia, & C. Uggen. "Out and Down: Incarceration and Psychiatric Disorders." Journal of Health & Social Behavior, 2011, 53(4), pp. 448-464.
Shaheen, G., & J. Rio. "Career Mapping for Disadvantaged Job Seekers." New York, NY: Corporation for Supportive Housing, Chronic Homelessness Employment Technical Assistance Center, November 2006.
Shen, C., M. Smyer, K. Mahoney, L. Simon-Rusinowitz, J. Shinogle, J. Norstrand, E. Mahoney, C. Schauer, & P. del Veccio. "Consumer-Directed Care for Beneficiaries with Mental Illness: Lessons from New Jersey's Cash and Counseling Program." Psychiatric Services, 2008, 59(11).
Siegwarth, A., and C. Koyanagi. "The Affordable Care Act: Improved Options for North Carolinians with Mental Illnesses." North Carolina Medical Journal, 2012, 73(3), pp. 240-243.
Smith, G., C. Kennedy, S. Knipper, J. O'Brien, & J. O'Keefe. "Using Medicaid to Support Working Age Adults with Serious Mental Illnesses in the Community: A Handbook. U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy, 2005. Available at http://aspe.hhs.gov/daltcp/reports/handbook.htm.
Solomon, P., and J. Draine. "The State of Knowledge of the Effectiveness of Consumer Provided Services." Psychiatric Rehabilitation Journal, 25(1), pp. 20-27.
Social Security Administration. "Annual Statistical Report on the Social Security Disability Insurance Program, 2010," SSA Publication #13-11827, August 2011a. Available at http://www.ssa.gov/policy/docs/statcomps/di_asr/2010/di_asr10.pdf.
Social Security Administration. "SSI Annual Statistical Report, 2010." SSA Publication #13-11827, August 2011b. Available at http://www.ssa.gov/policy/docs/statcomps/ssi_asr/2010/ssi_asr10.pdf.
Social Security Administration. "Continued Medicaid Eligibility (section 1619(B))." n.d. Available at http://www.socialsecurity.gov/disabilityresearch/wi/1619b.htm. Accessed January 15, 2013.
Social Security Administration. "Understanding Supplemental Security Income SSO Eligibility Requirements--2012 Edition." Last modified December 27, 2012. Available at http://www.socialsecurity.gov/ssi/text-eligibility-ussi.htm. Accessed February 1, 2013.
Stapleton, D., S. Liu, D. Phelps, & S. Prenovitz. "Work Activity and Use of Employment Supports Under the Original Ticket to Work Regulations: Longitudinal Statistics for New Social Security Disability Insurance Beneficiaries," Washington, DC: Mathematica Policy Research, December 2010. Available at http://www.ssa.gov/disabilityresearch/documents/TTW5_7_DICohort_rev.pdf.
Stegman, M., & R. Weathers. "The Impact of Supplemental Rehabilitation on the Labor Market Activity of Social Security Disability Insurance (SSDI) Beneficiaries." Under Review.
Substance Abuse and Mental Health Services Administration. "SAMHSA Grant Awards by State 2012/2013." 2012. Available at http://www.samhsa.gov/Statesummaries/index.aspx. Accessed January 14, 2013.
Substance Abuse and Mental Health Services Administration."2010-2011 National Survey on Drug Use and Health Model-Based Estimates 50 States and the District of Columbia." Available at http://www.samhsa.gov/data/NSDUH/2k11State/NSDUHsaeTables2011.pdf. Accessed January 3, 2013.
Substance Abuse and Mental Health Services Administration, "2011 Mental Health National Outcome Measures (NOMS): CMHS Uniform Reporting System." Available at http://www.samhsa.gov/dataoutcomes/urs/. Accessed July 10, 2013.
Substance Abuse and Mental Health Services Administration, "State Estimates of Substance Abuse and Mental Disorders from the 2010-2011 NSDUH: Results and Detailed Tables." Available at http://www.samhsa.gov/data/NSDUH/2k11State/NSDUHsae2011/Index.aspx.
Thompkins, A., T. Honeycutt, C. Gill, J. Mastrianni, & S. Bailey."To Apply or Not To Apply: The Employment and Program Participation Experiences of Social Security Disability Insurance Applicants and Non-Applicants." DRC Working Paper Series.Washington, DC: Mathematica Policy Research, forthcoming.
Tompa, E., C. de Oliveira, R. Dolinschi, & E. Irvin. "A Systematic Review of Disability Management Interventions with Economic Evaluations." Journal of Occupational Rehabilitation, 2008, 18(1), pp. 16-26.
Twamley, E.W., D.V. Jeste, & A.F. Lehman. "Vocational Rehabilitation in Schizophrenia and Other Psychotic Disorders: A Literature Review and Meta-Analysis of Randomized Controlled Trials." Journal of Nervous & Mental Disease, 2003, 191(8), pp. 515-523.
Twamley, E.W. & J.M. Narvaez. "Supported Employment for Middle-Aged and Older People with Schizophrenia." American Journal of Psychiatric Rehabilitation, 2008, 11(1), pp. 76-89.
U.S. Department of Education, Rehabilitation Service Administration. "Supported Employment." Available at https://rsa.ed.gov/programs.cfm?pc=se. Accessed January 12, 2013.
U.S. Department of Health and Human Services, Center for Medicare and Medicaid Services. "Individuals with Disabilities." Available at http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Population/People-with-Disabilities/Individuals-with-Disabilities.html. Accessed February 1, 2013.
U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services. "Medicaid: Eligibility." Available at http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Eligibility/Eligibility.html. Accessed January 10, 2013.
U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services, Center for Medicaid, CHIP and Survey and Certification. "Health Homes for Enrollees with Chronic Conditions."Baltimore, MD: Centers for Medicare and Medicaid Services, 2010a.
U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services, Center for Medicaid, CHIP and Survey and Certification. "CMCS Informational Bulletin: Updates to the 1915(c) Waiver Instructions and Technical Guide Regarding Employment and Employment Related Services".U.S. Department of Health and Human Services, 2011.
U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services. "Medicaid: Section 1115 Demonstrations."Available at http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Waivers/1115/Section-1115-Demonstrations.html. Accessed January 11, 2013.
U.S. Department of Health and Human Services. "Essential Health Benefits, Actuarial Value, and Accreditation Standards: Ensuring Meaningful, Affordable Coverage." 2012. Available at http://www.healthcare.gov/news/factsheets/2012/11/ehb11202012a.html. Accessed January 9, 2013.
U.S. Department of Health and Human Services. "Key Features of the Affordable Care Act, by Year." Available at http://www.healthcare.gov/law/timeline/full.html. Accessed January 10, 2013.
U.S. Department of Health and Human Services, National Institutes of Health, National Institute of Mental Health. "Recovery After an Initial Schizophrenia Episode (RAISE): A Research Project of the NIMH." Available at http://www.nimh.nih.gov/health/topics/schizophrenia/raise/index.shtml. Accessed January 3, 2013.
U.S. Department of Labor, Employment and Training Administration Advisory System. "Announcement of American Job Center Network. Advisory: Training and Employment Guidance Letter No. 36-11." June 14, 2012.
U.S. Department of Veterans Affairs. "Compensated Work Therapy."2009. Available at http://www.cwt.va.gov/veterans.asp. Accessed January 15, 2013.
U.S. Department of Veterans Affairs. "Employment Opportunities for Veterans."Available at http://www.va.gov/HOMELESS/employment.asp. Accessed January 15, 2013.
Vantil, L., D. Fikretoglu, T. Pranger, S. Patten, J. Wang, M. Wong, M. Zamorski, P. Loisel, M. Corbiere, N. Shields, J. Thompson, & D. Pedlar. "Work Reintegration for Veterans with Mental Disorders: A Systematic Literature Review to Inform Research." Physical Therapy, 2012.
van Oostrom, S.H., M.T. Driessen, H.C.W. de Vet, R.L. Franche, E. Schonstein, P. Loisel, W. van Mechelen, & J.R. Anema. "Workplace Interventions for Preventing Work Disability."Cochrane Database of Systematic Reviews, 2009, 2.
Vuori, J., S. Toppinen-Tanner, & P. Mutanen. "Effects of Resource-Building Group Intervention on Career Management and Mental Health in Work Organizations: Randomized Controlled Field Trial." Journal of Applied Psychology, 2012, pp. 273-286.
Westbrook, J.D., C. Nye, & F. Martin. "Effectiveness of Adult Employment Assistance Services for Persons with Autism Spectrum Disorders". Campbell Systemic Reviews, 2012.
Williams, R.M., M.G. Westmorland, C.A. Lin, G. Schmuck, & M. Creen."Effectiveness of Workplace Rehabilitation Interventions in the Treatment of Work-Related Low Back Pain: A Systematic Review." Disability & Rehabilitation, 2007, 29(8), pp. 607-624.
Wittenburg, D., A. Rangarajan, & T. Honeycutt. "The United States Disability System and Programs to Promote Employment for People with Disabilities." Revue Française des Affaires Sociales, 2008, pp. 111-136.
Whalen, D., G. Gimm, H. Ireys, B. Gilman, & S. Croake. "Demonstration to Maintain Independence and Employment Final Report." Washington, DC: Mathematica Policy Research, 2012.
Wong, K.K., R. Chiu, B. Tang, D. Mak, J. Liu, & S.N. Chiu. "A Randomized Controlled Trial of a Supported Employment Program for Persons with Long-Term Mental Illness in Hong Kong." Psychiatric Services, January 2008, 59(1), pp. 84-90.
Notes
-
IPS programs have been formally assessed regarding adherence, or fidelity, to these evidence-based principles. We use "evidence-based SE" rather than "IPS" in this report because programs we examined may not necessarily have been assessed for fidelity, although they are built upon the evidence-based principles (Bond et al. 2012).
-
See http://www.dartmouth.edu/~ips/page3/page10/page10.html, accessed on January 6, 2013.
-
The Progressive Goal Attainment Program is a flexible step-based program designed to reduce psychosocial barriers to rehabilitation progress, promote reintegration into life-role activities, increase quality of life, and facilitate return-to-work. See http://www.pdp-pgap.com/pgap/en/index.html, accessed January 7, 2013
-
Because study participants were not randomly assigned into groups of disclosers and non-disclosers, the study is quasi-experimental and may lead to selection bias.
-
Because these analyses are based on those who obtained employment or enrolled in school, which depends in part on the randomized group assignment, these results are quasi-experimental and may be subject to selection bias.
-
See http://store.samhsa.gov/product/Supported-Education-Evidence-Based-Practices-EBP-Kit/SMA11-4654CD-ROM, Building Your Program, accessed July 15, 2013.
-
The authors do not report whether employees received public or private disability benefits or workers' compensation.
-
Early contact was not defined.
-
Early contact was not defined.
-
In general, ergonomic visits to the worksite consist of an evaluation by an ergonomist or physiotherapist to provide practical instruction to the employee on appropriate ways of using the back or workplace adaptations, but the nature of the ergonomic interventions varied by study site.
-
Work hardening is defined as an individualized job-specific program using simulated or real work tasks, such as lifting, progressively graded conditioning exercises based upon the individual's measured tolerance, with the goal of RTW. See http://www.lni.wa.gov/ClaimsIns/Files/ReturnToWork/WhStds.pdf.
-
The Rehabilitation Act defines SE as, " competitive work in integrated work settings, or employment in integrated work settings in which individuals are working toward competitive work, consistent with the strengths, resources, priorities, concerns, abilities, capabilities, interests, and informed choice of the individuals, for individuals with the most significant disabilities (1) for whom competitive employment has not traditionally occurred; or (2) for whom competitive employment has been interrupted or intermittent as a result of a significant disability; and (3) who, because of the nature and severity of their disability, need intensive supported employment services in order to perform such work."
-
At-risk groups are defined below.
-
We appreciate the support of SSA's Disability Research Consortium, which provided additional funding for this project.
-
See http://store.samhsa.gov/product/Supported-Education-Evidence-Based-Practices-EBP-Kit/SMA11-4654CD-ROM, Building Your Program, p. 15, accessed July 15, 2013.
-
Several states have used Medicaid to fund Supported Employment in ways that Supported Education could be incorporated. For example, one state offered employment-related services that included developing skills to reduce or overcome the symptoms of mental illness, planning and managing activities to achieve outcomes, and developing supportive contacts in school. Another state provided employment-related services such as supportive counseling and problem-focused interventions in whatever setting was required to enable consumers to manage the symptoms of their illness. While these examples of using Medicaid are not directly related to Supported Education, they are examples of how providers may define service provision to support the Medicaid mission. See http://aspe.hhs.gov/daltcp/reports/handbook.htm.
-
42 CFR 440.130(d).
-
The ACA extended the MFP demonstration through September 2016, added $2.25 billion in funding ($450 million for each fiscal year from 2010-2016), and broadened the eligibility criteria to include individuals who live in an institution for more than 90 consecutive days (HHS n.d. b).
-
An "individual with a severe disability" is one who has "a severe physical or mental impairment that seriously limits one or more functional capacities (such as mobility, communication, self-care, self-direction, interpersonal skills, work tolerance, or work skills) in terms of an employment outcome, whose VR can be expected to require multiple VR services over an extended period of time," and who has one or more disabilities resulting from one of a range of conditions (34 CFR § 369.4).
-
34 CFR 363.3.
-
34 CFR 363.4.
-
Grandfathered plans are exempt from this provision, meaning that individuals covered by a plan with grandfathered status may remain without mental health benefits.
-
The ACA exempts employers with fewer than 100 employees from this mandate, replacing the previous exemption of employers with fewer than 50 employees.
-
Federal regulations define individuals with disabling mental disorders to include: "children with serious emotional disturbances and adults with serious mental illness; individuals with serious and complex medical conditions, individuals with chronic substance abuse disorders; individuals with a physical, intellectual or developmental disability that significantly impairs their ability to perform one or more activities of daily living, or individuals with a disability determination based on Social Security criteria or in States that apply more restrictive criteria than the Supplemental Security Income program, the State plan criteria." See https://s3.amazonaws.com/public-inspection.federalregister.gov/2013-16271.pdf (page 534).
-
See http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SMD-12-003.pdf.
-
In most states, eligibility for SSI automatically qualifies an individual for Medicaid. To be eligible for SSI based on disability status, an individual must have a physical or mental impairment which results in an inability to perform any substantial gainful activity (SGA), and can be expected to result in death or has lasted or will be expected to last for at least 12 months (SSA 2012). In 2013, SGA is defined as work that results in earnings averaging more than $1,040 each month. However, some states (known as 209(b) states) use more restrictive eligibility criteria beyond SSI eligibility (HHS n.d.). In general, individuals who do not receive SSI but seek Medicaid coverage based on disability must prove they have some type of impairment that prevents them from performing SGA for at least a year.
-
1915(d) waivers provide HCBS to individuals 65 and older who would otherwise require institutionalization. The 1915(e) waivers fund HCBS to children under age 5 who were infected with HIV at birth, currently have AIDS or were dependent on heroin, cocaine, or PCP at birth, as long as those children would otherwise require institutionalization (Social Security Act n.d.). Section 1115 Demonstrations are experimental or pilot Medicaid programs which are approved for a five-year period and can be renewed for an additional three years (HHS, CMS n.d.).
-
California, Colorado, Connecticut, Iowa, Idaho, Louisiana, Nevada, Oregon, Washington, and Wisconsin have an approved 1915(i) state option. See http://kff.org/medicaid/state-indicator/section-1915i-home-and-community-based-services-state-plan-option/.
-
Part of a project funded by the National Institute on Disability and Rehabilitation Research, this registry of systematic reviews includes 105 reviews on disability and rehabilitation topics culled from major registries, unpublished sources, and open-access sources. See http://www.ktdrr.org/cgi-bin/lib_systematic_search.cgi.
Appendices
APPENDIX A: Evidence Tables
| TABLE A.1. Evidence for Improving Employment Outcomes Through SE: Studies Included in Systematic Reviews | ||||||
|---|---|---|---|---|---|---|
| Systematic Review Source(s) |
Study Author, Countrya |
Study Designa |
Intervention (sample size)b |
Comparison (sample size)b |
Notable Sample Characteristicsb |
Results (intervention vs. comparison)a |
| Twamley et al. (2003) | Bond et al. (1995), USA | RCT | SE (N=74, incl. both T and C groups) | 4 months pre-vocational training, followed by SE | Avg. age: 35 Schizophrenia spectrum: 66% >HS education: 59% |
During 12 months--
|
| Bond et al. (2008) | Latimer et al. (2006), Canada | RCT | IPS (N=75) | Traditional vocational services (N=74) | Avg. age: 40 Schizophrenia spectrum: 68% in T, 84% in C >12 years education: 43% |
During 12 months--
|
| Bond et al. (2008) | Twamley et al. (2008), USA | RCT | IPS (N=28) | Referral to VR (N=22) | Avg. age: 50 All participants were 45 or older Schizophrenia spectrum: 100% |
During 12 months--
|
| Twamley et al. (2003) | Bond & Dincin (1986), USA | RCT | "Accelerated" transitional employment (immediate placement in paid work group) (N=107 across T and C groups) | "Gradual" transitional employment | Age: 68% >21 Schizophrenia spectrum: 55% >HS education: 80% |
During 15 months--
|
| Bond et al. (2008) | Burns et al. (2007), European cities | RCT | IPS (N=156) | Traditional vocational services (N=156) | Not reported in systematic review | During 18 months--
|
| Twamley et al. (2003) Bond et al. (2008) |
Drake et al. (1996), USA | RCT | IPS (N=73) | Non-integrated group skills training (N=67) | Avg. age: 37 Schizophrenia spectrum: 47% >HS education: 74% |
During 18 months--
|
| Twamley et al. (2003) Bond et al. (2008) |
Drake et al. (1999), USA | RCT | IPS (N=74) | Sheltered workshop (N=76) | Participants were from an inner city Avg. age: 39 Schizophrenia spectrum: 67% >HS education: 50% |
During 18 months--
|
| Twamley et al. (2003) | McFarlane et al. (2000), USA | RCT | FACT+ vocational specialist (provided for first 1-2 months) (N=37) | Enhanced VR (counselor ensured and monitored service use) (N=32) | Avg. age: 33 Schizophrenia spectrum: 65% >HS education: 89% |
During 18 months--
|
| Bond et al. (2008) | Wong et al. (2008), Hong Kong | RCT | IPS (N=46) | Stepwise conventional vocational services (N=46) | Avg. age: 33 Schizophrenia spectrum: 32% >HS education: 22% |
During 18 months--
|
| Bond et al. (2008) | Bond et al. (2007), USA | RCT | IPS (N=92) | Diversified placement approach (N=95) | Avg. age: 40 Schizophrenia spectrum: 63% |
During 24 months--
|
| Bond et al. (2008) | Gold et al. (2006), USA | RCT | IPS+ACTd (N=66) | Sheltered workshop (N=77) | Age: 77% ages 26-45 (T), 64% (C) Schizophrenia spectrum: 74% (T), 62% (C) >HS education: 52% |
During 24 months--
|
| Twamley et al. (2003) Bond et al. (2008) |
Lehman et al. (2002), USA | RCT | IPS (N=113) | Psychosocial rehabilitation (with vocational services for 33%) (N=106) | Avg. age: 42 Schizophrenia spectrum: 75% >HS education: 51% |
During 24 months--
|
| Twamley et al. (2003) | McFarlane et al. (1996), USA | RCT | FACT (N=37) | ACT + crisis family intervention (N=31) | Avg. age: 30 Schizophrenia spectrum: 100% >HS education: 51% |
During 24 months--
|
| Bond et al. (2008) | Mueser et al. (2004), USA | RCT | IPS (N=68) | (i) Brokered SE, (ii) Psychosocial rehab, or (iii) groups (i) and (ii) combined (N=136) | Avg. age: 42 Schizophrenia spectrum: 77% |
During 24 months--
|
| Twamley et al. (2003) | Okpaku et al. (1997), USA | RCT | Case management + vocational specialist (provided for first 4 months) (N=73) | Services-as-usual (N=79) | All participants were applying for or receiving SSI/SSDI. Avg. age: 37 Schizophrenia spectrum: 38% Avg. education: 11.5 years |
During 24 months--
|
| Twamley et al. (2003) | Chandler et al. (1996), USA | RCT | ACT+ vocational specialist (N=102 urban, 115 rural) | Community mental health services-as-usual (N=108 urban, 114 rural) | Age: 30% over age 45 Schizophrenia spectrum: 61% |
During 36 months--
|
NOTES: Results based on subsamples of those who worked competitively are likely biased upwards. Unless otherwise indicated, Bond et al. (2008) and Twamley et al. (2003) did not report statistical significance. Bolded studies indicate that the study reported statistically significant intervention-comparison differences for one or more outcomes.
|
||||||
| TABLE A.2. Evidence for Improving Employment Outcomes Through SE: Studies Reviewed by Mathematica | |||||
|---|---|---|---|---|---|
| Study Author, Country |
Study Design |
Intervention (sample size) |
Comparison (sample size) |
Notable Sample Characteristics |
Results (intervention vs. comparison) |
| Macias et al. (2006), USA | RCT | SE+ACT (N=63) | Clubhouse (N=58) | Sample characteristics and results represent the participants who expressed interest in working Avg. age: 36 years old in ACT, 40 years old in clubhouse Schizophrenia spectrum: 60% ACT, 43% clubhouse >HS education: 61% |
During 24 months--
|
| Frey et al. (2011), USA | RCT | IPS + medication management (N=1,004) | List of available local and national services (N=1,051) | Participants were SSDI beneficiaries Avg. age: 47 Schizophrenia spectrum: 30% >HS education: 88% |
During 24 months--
|
| Cook et al. (2005b), USA | Summary of cross-site results from studies of EIDP, a large, multisite RCT | Several SE models including IPS, FACT, ACT, and clubhouse | Services-as-usual or weaker versions of the intervention | 1,273 participants were randomly assigned in 7 states Avg. and median age: 38 Schizophrenia spectrum: ~50% >HS education: ~67% |
During 24 months--
|
| Bond et al. (2008),a USA, Canada, Europe, Hong Kong | Systematic review with meta-analysis | IPS | C groups received treatment as usual (typically referral to VR) or alternative vocational models; 2 studies compared IPS to non-integrated SE | Reviewed 11 RCTs with high model fidelity Eligibility criteria across studies: adults who met criteria for SMI, unemployed at intake, expressed desire to work (in all but 1 of the studies), absence of significant medical condition | Results from pooled analysis (study periods differed)--
|
| Campbell et al. (2009),a USA | Non-systematic review with meta-analysis | IPS (N=307) | Group skills training, enhanced VR, psychosocial rehabilitation, or diversified placement (N=374) | Reviewed 4 RCTs of high-fidelity IPS modelsb | Effect sizes calculated based on 13 demographic or clinical characteristics for 3 outcomes ranged from: 0.67-1.42 for competitive employment; 0.50-1.06 for weeks worked; and 0.47-1.09 for job tenure Effect sizes were significant (p<0.05) for all but 2 subgroups--those who are married or living with a partner, and those who are divorced, separated or widowed--and most were considered large (>0.70) There were few instances in which 1 subgroup appeared to benefit more from IPS than another group. For example, those who had more than a high school degree showed less improvement with IPS than those with less education |
| Twamley et al. (2003),a USA | Systematic review with meta-analysis | SE, IPS | Pre-vocational training, skills training, sheltered workshop, VR | Reviewed 6 RCTs of SE | Results from pooled analyses (study periods differed)--
|
NOTES: Unless otherwise indicated, statistical significance was not reported. Results based on subsamples of those who worked competitively are likely biased upwards. Underlined studies indicate that the study reported statistically significant intervention-comparison differences for one or more outcomes.
|
|||||
| TABLE A.3. Evidence for Improving Employment Outcomes of Long-Term Clients of Traditional Mental Health Services | |||||
|---|---|---|---|---|---|
| Study Author, Country | Study Design | Service Type (sample size) |
Comparison (sample size) |
Notable Sample Characteristics |
Results |
| Vantil et al. (2012), USA | SR | Interventions to maximize reintegration of workers with mental disorders into the workforce | 97 observational or experimental studies | 32 of 97 studies concerned reintegration; 10 of them were conducted in populations of veterans | Limited knowledge exists about how to reintegrate people with mental disorders into a new workplace after an absence of more than a year. Knowledge specific to veterans is even more limited. |
| Davis et al. (2012), USA | RCT | IPS model described in A Working Life for People With Severe Mental Illness (N=42) | Standard VR Program (N=43) | Veterans at the Tuscaloosa VA Medical Center ages 19-60 with a diagnosis of PTSD, a medical clearance to work, and who are currently unemployed and interested in competitive employment | The study group was 2.7 times more likely to gain competitive employment. Other employment outcomes, including time worked and total earnings, also favored the study group. These findings were statistically significant and are consistent with previously reported advantages of IPS over traditional VR programs. |
| Michalopoulos et al. (2011), USA Stegman and Weathers (2012), USA | RCT | SSDI beneficiaries with no health insurance received health insurance, medical care management, employment and benefits counseling and PGAP for new SSDI recipients; N=611; 22% had mental disorders, including individuals with psychiatric disabilities | AB group received only health benefits package (N=400) and new SSDI recipients with no intervention (N=986) | Newly entitled SSDI beneficiaries who were approved at their initial medical determination ages 18-54 with at least 18 months before the start of their entitlement to Medicare and who resided in 1 of the 53 metropolitan areas included in the demonstration | The AB Plus group participated in vocational services at a greater rate during all 3 years of follow-up, and was employed at a greater rate and earned more on average during the second year after random assignment. These results disappeared at the third year follow-up. Results were statistically significant. |
| Burt (2012), USA | QED | Housing assistance, employment case management, case coordination by an employment specialist, work supports such as training and uniforms, and linkages to workforce development centers provided at 1 of 3 LA County community mental health centers (N=56) | Homeless individuals with SMI receiving non-program services at one of the other 15 LA County community mental health centers (N=415) | All participants qualified for county mental health services, usually with a diagnosis of schizophrenia or affective disorder, and were homeless at enrollment. Propensity score matching was used to compare groups. | The T group had an employment participation rate (57% vs. 22%) and competitive employment rate (27% vs. 13%) more than double that of the comparison group. T group participants were more likely to work FT rather than PT and less likely to have had no employment at all while in the program. Of those who did gain employment, the T group took fewer days to do so and worked more days in competitive employment after they did. Approximately half of the overall days worked by T group participants were in competitive employment. Some but not all of the observed employment outcomes may, in fact, be attributable to improved housing outcomes rather than to a specific employment intervention. |
| Harpaz-Rotem et al. (2011), USA | QED | Residential treatment longer than 30 days, including a variety of clinical and rehabilitation services available at 11 HWVP facilities (N=217) | Identical residential treatment that lasted less than 30 days (N=234) | Homeless female veterans who had been receiving VA health services for less than 6 weeks and had psychiatric and or addiction disorders | The T group had significantly more days worked on average. Treatment was also associated with significantly improved clinical outcomes in a variety of non-employment domains. Because the services offered at the HWVPs varied, it is theorized that the provision of housing, rather than specific services, was the key factor in improving employment outcomes. |
| Gao et al. (2009), USA | Pre-post | In-house SE services (N=60) | n/a | Clients with SMI at a supportive housing agency in New Jersey, including individuals with long histories of hospitalizations | The competitive employment rate doubled to 26% after 12 months and remained above 50% after 24 months. Another 18% had returned to school or participated in job training at the end of 3 years. |
| Shaheen and Rio (2006) | Descriptive | Career mapping, which identifies strengths, gifts, and capacities of participants to reveal concrete strategies for addressing barriers to employment (N=45) | n/a | Homeless clients with disabilities, not all of whom had psychiatric disabilities, who want to work | Of 45 participants, over 18 months, 25 obtained jobs consistent with their person-centered plan. Consistent with their "zero reject" approach, these were all chronically homeless individuals, defined as being homeless continuously for more than a year or for having experienced at least 4 episodes of homelessness in the past 3 years, and having a disabling condition. |
| Marrone (2005), USA | Descriptive | Blend of SE and ACT (N=791) | n/a | Homeless individuals in Vancouver, Washington, identified in shelters and at transitional housing sites with a "zero reject" approach | The goal for the 5-year program was to engage 250 clients, develop 175 personal career plans or vocational profiles, and help 75 participants secure employment. After 39 months, 791 clients had been engaged, 543 vocational profiles developed, and 129 participants had secured employment. |
| Rosenheck and Mares (2007), USA | Pre-post/ implementation study | IPS (N=321) | Services received prior to implementation of IPS (N=308) | Homeless veterans who were not receiving VA health services, expressed interest in seeking competitive employment, and were diagnosed as having a psychiatric or substance abuse problem | Controlling for baseline differences, the post-implementation group engaged in an average of 15% more days of competitive employment over the 2-year follow-up period. The study's authors conclude that a low-intensity training approach can successfully implement an IPS program in a system previously unfamiliar with the approach and show improved employment outcomes. |
| Anthony (2006), USA | Descriptive | SE (N=37) | Individuals with severe and persistent mental illness who received SE services but had no forensic involvement (N=1,236) | No significant background differences between those with recent forensic involvement and those without. Those with forensic involvement were more likely to have worked in the previous 5 years, less likely to have a diagnosis of schizophrenia, and to have had significantly higher levels of positive and general symptoms. | In this unpublished and exploratory analysis, forensic involvement was a non-significant indicator for all employment outcomes for individuals with severe and persistent mental illness receiving SE services in the EIDP. The implication is that SE may be an effective employment intervention for the forensically involved because that population enjoyed the same employment gains in the EIDP as those without forensic involvement. |
| NOTE: Underlined studies indicate that the study reported statistically significant intervention-comparison differences for one or more outcomes. T=treatment (group); PT=part-time; FT=full-time. |
|||||
| TABLE A.4. Evidence for Improving Employment Outcomes of Individuals At Risk of Job Loss | |||||
|---|---|---|---|---|---|
| Study Author, Country |
Study Design |
Service Type (sample size) |
Comparison (sample size) |
Notable Sample Characteristics |
Results |
| Fossey et al. (2010), Canada | SR | This review sought to identify implications from qualitative studies investigating the employment-related views of people with persistent mental ill health to guide further development of employment supports for them. | 20 studies were included for qualitative metasynthesis. | Included studies were conducted in the USA, Canada, Australia, England, and New Zealand. Participants were employed in wide-ranging jobs. | Support within the workplace can affect job satisfaction, job retention, job stress, decisions regarding disclosure of psychiatric disabilities, and decisions to leave jobs. The authors found that employment has varied meanings, benefits, and drawbacks; strategies for maintaining employment and mental health are important and require ongoing active self-management; supports in and out of the workplace are helpful; and employment barriers are partially systematic. |
| Furlan et al. (2011), Canada | SR | The review examined interventions or programs that could be implemented in workplaces to improve workers' depression and reduce associated productivity losses. | 14 articles on 12 studies were included; 10 of the 12 were RCTs and 2 were non-randomized studies. 4 studies were conducted in The Netherlands, 4 in the USA, and 1 each in Canada, Finland, Denmark, and Japan. | Interventions were psychological (2 studies), enhanced primary care (4), psychiatry plus occupational therapy (1), enhanced occupational physician roles (2), integrated care management (2), exercise (1), and worksite intervention (1). | Evidence from all included studies were considered "very low" quality because: (1) all included studies were judged to be at a high risk of bias; (2) evidence for specific interventions was always based on data from 1 study; (3) the population included in the studies was often not considered generalizable to the population of interest for this review; and (4) there was imprecise data for all primary outcomes because in all instances only 1 study provided evidence. The authors concluded they cannot recommend any 1 intervention, and instead recommend future research. The review also found intervention savings to employers ranged from $503 to $5,136 per worker. Savings to society ranged from an incremental cost-effectiveness ratio of -736 Euros to an incremental cost per QALY above usual care of $36,467. |
| Nieuwenhuijsen et al. (2008), Holland | SR | The review examined work-directed and worker-directed interventions for reducing work disability of depressed workers. | 11 RCTs | No work-directed interventions were included. Interventions were pharmacological (4), psychological (2), and combinations of the two (5). | The authors could not find any high quality studies of employer-level interventions. The review found limited evidence that clinical intervention can reduce sickness absence from work in depressed people. The authors conclude that depressed employees require work supports and accommodations in addition to clinic treatment in order to improve employment outcomes. |
| Krupa (2007), Canada | NSR | The review examined employment interventions for individuals who experience mental illness. | The author developed a framework of individual-level intervention categories. | Employer-level interventions include routine screenings, education/awareness campaigns, and developing organizational frameworks conducive to good mental health. | The author did not find high-level evidence for employer-level interventions. There was more support for individual-level interventions, including clinical treatment, social network development, and reasonable job accommodations. |
| Lauber and Bowen (2010), UK | NSR | The review examined interventions to promote keeping people with affective disorders working or to help them return to work. | The study reviewed interventions for people in 5 categories: mental health, people with an existing workplace, people without a workplace, employer-level interventions, and people with other than mental health problems. | Interventions included clinical treatment, case managers providing employees with appropriate supports, supervisor support, social support, and education and training. | The authors found a wealth of studies reporting on interventions to assist employees with affective disorders, but few that report employment outcomes. The research is even weaker for employer-level interventions. The authors conclude there is a large gap in the research evidence on this topic. |
| Bohman et al. (2011), USA | RCT | The study examined Texas' DMIE program. "wrap-around" health services (N=888). | Regular health care through Texas' Harris County Hospital District (N=697) | Participants were low-income, working adults; predominately female (77%), middle-aged (mean age 47), and minority (40% African American, 30% Hispanic); 11% diagnosed with SMI. | Intervention participants were twice as likely to make any mental health visit (12% vs. 6%, significant at 0.01), and less likely to receive SSI/SSDI (6% vs. 8%). Intervention participants displayed no significant difference in employment, earnings outcomes, or mean SF-12 MCS scores. |
| Linkins et al. (2011), USA | RCT | The study examined Minnesota's DMIE program: a comprehensive set of health, behavioral health, and employment-support services, coordinated through a navigator (N=888). | Usual care (N=267) | Participants were working at least 40 hours/month, had mental illness diagnosis, and were not eligible for other state-sponsored public programs. | The intervention group maintained or improved ADL functioning compared to the C group. There was no significant difference in employment outcomes between groups, although lower-functioning participants from the C group displayed lower earnings than lower-functioning T group members. Participants in the intervention who were more engaged with the program displayed significant improvements in mental health status. |
| Whalen, et al. 2012. (USA) | RCT | The DMIE program, interventions providing medical benefits and financial assistance for health care, although the specific packages of services varied in each of four states (N=2,125). Only Minnesota and Texas intentionally focused on people with mental health. | Usual care, although control conditions vary by state (N=1,299) | Sample characteristics varied by state. Participants in all states were primarily female. Minnesota, which focused specifically on individuals with mental health issues, had the lowest mean mental SF-12 score (35.0). | The evaluation of the DMIE program as a whole found no significant differences between the percent of T group participants and C group participants not employed by the end of the study period (which was either 12 or 24 months, depending on the state). The combination of Minnesota and Texas participants saw an insignificant increase in employment of 0.2%. The authors note that the only states to show statistically significant reductions in dependence on SSA benefits focused their interventions on a population with behavioral health problems. |
| Vuori et al. (2012), Finland | RCT | The study examined in-company training program for employees of 17 organizations with the goal of enhancing career-management, mental health, and job retention (N=369). | Printed information about career and health-related issues (N=349) | Participants were employees at medium-sized and large-sized organizations. Mean age was 50.1 years, 88% were female, and most had a degree beyond high school (60%). | At the 7-month follow-up period, the intervention group displayed significantly decreased depressive symptoms and intentions to retire compared with the C group. |
| Adler et al. (2006), USA | OS | This was a 3-year longitudinal observational study of 286 patients with DSM-IV major depressive disorder and/or dysthymia | The comparison group included 93 individuals with rheumatoid arthritis, and 193 depression-free healthy control subjects. | At baseline, 25% of the depression group met the screening criteria for dysthymia and 75% met criteria for major depressive disorder and double depression. Mean number of symptoms was 2.9 for the dysthymia group, 4.8 for major depressive disorder, and 4.6 for double depression. | Employees undergoing treatment for depression had worse job-performance scores than healthy employees even after demonstrating clinical improvements in symptom severity. Specifically, the study identified persistent deficits in performance of mental-interpersonal tasks, time management, output, and physical tasks. The study concludes that, although clinical interventions improve mental health, additional workplace interventions may be required to improve the performance of depressed employees. |
| Burton et al. (2007), USA | OS | This was a retrospective observational cohort study of 2,112 employees with a new episode of treatment with an antidepressant medication. | 1,301 employees adhered to acute-phase treatment, and 966 remained adherent to continuation-phase treatment. | The population was 76% female and 87% Caucasian; 1.8% of all employees had a short-term disability event due to depression/ anxiety in pre-index period. | Adherent employees were significantly less likely to have any short-term disability absence (8.8%) compared with non-adherent employees (12.7%). In the continuation-phase, 966 employees were adherent and 1,146 were non-adherent. Adherent employees were less likely to have any short-term disability absence than non-adherent employees (8.4% compared with 12%). Adherent employees were also less likely to have multiple short-term disability absences (0.9%) than non-adherent employees (2.1%). |
| Dewa et al. (2003) UK, Canada | OS | This was a retrospective observational cohort study of 1,281 employees at 3 major Canadian financial and insurance companies. The study examined adherence to treatment protocol. | Included employees had depression-related absences from work, used their prescription drug benefit during the study period, and did not have more than 1 short-term disability episode 1 year prior to baseline. | The study population was overwhelmingly female (88%), had a mean of 4.1 depression symptoms, and 46.5% had additional mental health conditions besides depression. | Employees who returned to work FT or PT reported significantly fewer symptoms than those who left employment or went on long-term disability benefits. Employees who went on long-term disability benefits were significantly less likely to fill any antidepressant prescriptions during a short-term episode (27.7%) than those who returned to work (47.3%) or those who left work and did not go onto long-term disability benefits (42.7%). An ordinary least squares regression model found that EI was significantly associated with a reduced length of disability episode (β=-24.1 days). |
| Chow (2012), USA | OS | As part of the EIDP program, people were randomly assigned to 1 of 2 employment-intervention programs deemed experimental condition or to a services-as-usual control condition. This study of reasonable accommodations followed 1,654 people in both intervention and C groups. | There were 370 participants reporting receiving at least 1 accommodation at work, and 1,284 reporting no accommodations. | Of the accommodations cohort, 49.2% reported only 1 accommodation. Those without accommodations were on average older (by 2 years), had a higher estimated wage (62 cents), and had a higher proportion of individuals experiencing economic burden at baseline. | Participants with job accommodations worked an average of 7.68 hours more per month than those without accommodations. Participants with accommodations tended to work for longer periods of time, with each accommodation decreasing the risk of job loss by 12.7%. Average job tenure for individuals in the no-accommodations group was 157.47 days; the accommodations group averaged 206.96 days. Participants in the no-accommodations group were much more likely to have a diagnosis of schizophrenia and to report symptoms of social withdrawal and social avoidance, and they earned 5% more. The latter finding may be due to discrimination against employees who disclosed a mental illness diagnosis. Participants who reported disclosure had a larger probability of reporting accommodations. A literature review included in the study located no high quality RCTs or well-controlled quasi-experimental studies measuring outcomes for reasonable accommodations for individuals with mental disabilities in the literature. |
| NOTE: Underlined studies indicate that the study reported statistically significant intervention-comparison differences for one or more outcomes. T=treatment (group); C=control (group); FT=full-time; PT=part-time. |
|||||
| TABLE A.5. Evidence for Improving Employment Outcomes After a FE of Psychosis Through EI | |||||
|---|---|---|---|---|---|
| Study Author, Country |
Study Design |
Service Type (sample size) |
Comparison (sample size) |
Notable Baseline Sample Characteristics |
Results (intervention vs. comparison) |
| Garety et al. (2006), England | RCT | Comprehensive EI services w/occupational therapist (Lambeth Early Onset team) (N=67) | Generic CMHS with occupational therapist (N=65) | Avg. age: 26 years old Schizophrenia spectrum: 69% |
18 months later--
|
| Fowler et al. (2009), England | QED | Comprehensive EI services with occupational therapist (SE mentioned) ("EI" N=102) | Generic CMHS ("no-EI" N=82); and generic mental health coupled with an SE worker ("partial EI" N=69). No vocational support mentioned. | Avg. ages: 22, 23, 25, for "EI," "No-EI," and "Partial EI" Schizophrenia spectrum: 69% in "EI," 43% in "No-EI" ("Partial EI" not reported) |
2 years later (as measured during assessment month)--
|
| Killackey et al. (2008), Australia | RCT | Comprehensive EI services with IPS (EPPIC) ("EI+IPS," N=20) | Comprehensive EI services with referral to VR and possibly vocational group meetings (EPPIC) ("Standard EI," N=21) | Avg. age: 21 years old Schizophrenia spectrum: 100% Avg. duration of illness: 14 months |
Baseline--
|
| Major et al. (2010), England | QED | Comprehensive EI services with SE (VIBE) (N=44, including 4 who declined VIBE treatment) | Comprehensive EI services, no vocational support mentioned (N=70) | Avg. age: 24 years old Schizophrenia spectrum: 63% |
Baseline--
|
| Rinaldi et al. (2010), England | Pre-post | Comprehensive EI services with IPS (N=166, 142, 106, 67 at 6, 12, 18, and 24-month follow-ups) | None | Median age: 22 years old Schizophrenia spectrum: 96% |
Baseline--
|
| Porteous and Waghorn (2007), New Zealand | Post-hoc | EI community mental health with IPS (N=225) | None | Age range: 14-27 | During 24 months--
|
| Henry et al. (2010), Australia | Post-hoc | Comprehensive EI services with SE/IPS (EPPIC) (N=361) | None | Avg. age: 22 years old Schizophrenia spectrum: 67% Median duration of untreated psychosis: 46 months |
Participants were re-interviewed an avg. of 7 years after enrollment--
|
| Nuechterlein et al. (2008a, 2008b), USA | RCT | IPS + group-training in work skills, with outpatient psychiatric treatment (N=69) | Referral to VR + group-training in medicine management and communication, with outpatient psychiatric treatment (N=18) | Avg. age: 25 years old Schizophrenia spectrum: 100% Avg. duration of illness, including prodromal symptoms: 25 months |
During the first 6 months--
|
NOTES: Underlined studies indicate that the study reported statistically significant intervention-comparison differences for one or more outcomes.
|
|||||
| TABLE A.6. Evidence for Improving Employment Outcomes of TAY with SED or SMI | |||||
|---|---|---|---|---|---|
| Study Author, Country |
Study Design |
Intervention (sample size) |
Comparison (sample size) |
Notable Sample Characteristics |
Results (intervention vs. comparison) |
| Burke-Miller et al. (2012), USA | RCT | Several SE models including IPS, FACT, and ACT (EIDP); (N=30 youth; 86 young adults; 533 older adults) | Services-as-usual or weaker versions of the intervention (N=51 youth, 82 young adults, 490 older adults) | Participants were located in 7 states Youth=18-24 years old Young adults=25-30 Older adults=31+ Avg. age: 38 Schizophrenia spectrum: ~50% |
During 24 months--
|
| Browne and Waghorn (2010), New Zealand | Post-hoc | SE based on IPS, but not integrated with mental health services (N=49) | None | Avg. age: 21 Schizophrenia spectrum: 6% |
During 24 months--
|
| Karpur et al. (2005), USA | QED | TIP (Steps-to-Success), includes vocational training (N=43, limited to those with 1 year of participation) | Two matched comparison groups: (i) young adults with EBD in same county (N=990); (ii) young adults without EBD in same county (N=61,285) | Avg. age: 19 at follow-up | After exiting with at least 1 year of participation --
|
| Haber et al. (2008), USA | Pre-post | TIP (Partnership for Youth Transition), limited to those with 1 year of participation (N=193). | None | Avg. age: 17 Psychotic disorder: 9% |
At baseline--
|
| Fraker et al. (2013), USA | RCT | Guideposts for Success-based, with SSA waivers (YTD) (N=400) | Standard SSA rules and community services (N=383) | High School juniors or seniors with SMI or SED | 1 of the 6 sites had a significant, positive impact of 9 percentage points on whether the youth had held a job; 2 had significant impacts on whether the youth had held a job (19 and 9 percentage points, respectively) and on total earnings (a difference of $524 and $306 in annual earnings, respectively). The mental health focused project had no significant impacts on these outcomes. |
| NOTES: Unless otherwise indicated, statistical significance was not reported. Underlined studies indicate that the study reported statistically significant intervention-comparison differences for one or more outcomes. FT=full time, PT=part-time, n.s.=difference is not significant. |
|||||
| TABLE A.7. Evidence on Other Services and Supports | |||||
|---|---|---|---|---|---|
| Study Author, Country |
Study Design |
Service Type (sample size) |
Comparison (sample size) |
Notable Sample Characteristics |
Results |
| McDermid et al. (2008), UK | LR | The review examined studies of social enterprises focused on individuals with psychiatric disabilities. | 41 studies were reviewed for design and mental health outcomes; 1 study used a rigorous design and examined the effects of social enterprise employment on mental health. | Some studies included individuals with disabilities, not necessarily psychiatric; some examined SE more generally. | The 1 study identified by the authors (McKeown et al. 1992) suggested that working at a social enterprise improved mental health outcomes. |
| Lanctot et al. (2012), Canada | QED | The study examined employees of social enterprises in Quebec. | Outcomes were collected for 67 individuals and compared with those from other studies of competitive employment. | Employees of social enterprises had longer job tenure (86.9% of employees of social firms were still employed 6 months later, and the average job tenure of those at the firms was 6 years and 6 months, compared with average job tenure of less than a year) and worked more hours per week (30.7 compared with 15) than other studies have found among individuals with psychiatric disorders. | |
| Revell et al. (2009), USA | QED | The study compared individuals whose VR case was closed due to self-employment with others whose cases were closed due to employment (3,246 vs. 195,805). | The sample was composed of individuals with disabilities, not necessarily psychiatric, whose VR cases were closed due to employment. | Individuals with cases closed in self-employment had higher earnings than those with cases closed for other employment. | |
| Doughty and Tse (2005), New Zealand | LR | The review examined 26 studies of consumer-run and consumer-led services. | Review was conducted in New Zealand but some studies were conducted in the USA | The authors conclude that the literature agrees that consumer-run and consumer-led services are at least as effective as similar services delivered in traditional ways, and may be more effective. | |
| Rogers et al. (2007), USA | RCT | The study examined the effects of participation in consumer-operated service programs on empowerment. | Individuals were randomized into T (920) and C (907) groups. The T group was offered consumer-operated service programs in addition to traditional services; the C group received only traditional services. | Participants in the consumer-operated service programs experienced larger gains in empowerment than the C group. An intent to treat analysis also showed small positive effects. | |
| Solomon and Draine (2001), USA | LR | The review found 14 studies of consumer-operated services, consumer partnership services, and consumers as employees, 8 of which (representing 6 programs) used rigorous designs. | The 2 rigorous studies of a consumer-run service program found that services provided by consumers were of the same quality as those provided by non-consumers. Participants in a self-help program focused on employment experienced gains in the likelihood of being employed and progress toward employment among those not employed, as well as higher earnings among those who were employed. |
||
| Schmidt et al. (2008), USA | RCT | The study examined the effects of case management teams that include a consumer. | 142 individuals were randomly assigned to case management teams with or without a consumer member. | The 2 groups were found to be equivalent on all outcomes, including retention in the program, acute care use, adherence to medication, service use, substance abuse, and housing stability. | |
| Hutchinson et al. (2006), USA | Pre-Post | The study focused on 77 individuals in a peer-support specialist training program. | Pre-data and post-data were collected on self-efficacy, attitudes about recovery, and empowerment for the 66 participants who completed training. | Study participants were volunteers enrolled in the program. | 86% of study participants completed training, 80% of those were employed directly by the training agency, and 89% of them were still employed 12 months later. Among those who completed training, there were significant gains in self-efficacy, attitudes, and empowerment. |
| Shen et al. (2008), USA | QED | The study examined the effects of Cash and Counseling on non-elderly participants with mental illness. | 109 program participants were compared with a matched sample of 119 individuals who did not participate. | Controlling for background characteristics, the authors found that the T group was more satisfied with services, and the 2 groups were similarly likely to experience adverse health outcomes. | |
| Cook et al. (2008), USA | Pre-Post | The study examined outcomes for individuals participating in a self-directed care program. | Data was collected on 106 program participants in the year before enrollment and the year after. | Participants spent more days in the community and had higher functioning in the year after enrollment. There was no evidence of overspending. | |
| Cook et al. (2010), USA | LR/ Case Study | The report examined 8 IDA programs targeted toward individuals with psychiatric disabilities, and reviewed literature on IDA programs. | Many of the individuals using the IDA programs were able to successfully build savings to meet their goals. For those who were not successful, the barriers were not directly related to their having a psychiatric disability. No rigorous studies were found of the effectiveness of IDAs for individuals with disabilities. One study suggested that participants with disabilities had lower average monthly net deposits than those without. |
||
| Mowbray et al. (2005), USA | LR | The review found 8 studies of supported education, 2 of them of high quality. | Participants in supported education programs were more likely to enroll in post-secondary education. Pre-post studies found improved employment outcomes and decreased hospitalizations. One RCT found improved quality of life and self-confidence, and fewer social problems among participants. | ||
| Nuechterlein et al. (2008), USA | RCT | The study examined the effects of enrollment in a supported education program. | 69 individuals were randomly assigned to participate in supported education, or to be referred to VR services. | The study sample was mostly in their 20s and had recently experienced the onset of schizophrenia. | After 18 months, participants were about as likely to be enrolled in school, employed, or both. |
| Nuechterlein (2012), USA | RCT | This study reported outcomes for the investigation described in Neuchterlein et al. 2008. | 83% of participants returned to school or work within 6 months, compared with 41% of the C group; 92% of the T group was in education or employment for at least part of the following year. The T group also had longer time in school or a job. | ||
| NOTE: Underlined studies indicate that the study reported statistically significant intervention-comparison differences for one or more outcomes. T=treatment (group); C=control (group). |
|||||
| TABLE A.8. Evidence from Systematic Reviews of Employment Support and RTW Interventions for People with Other Disabilities | |||||
|---|---|---|---|---|---|
| Study Author, Country |
Study Design |
Interventions | Finance Mechanism |
Population | Key Findings |
| van Oostrom et al. (2009); USA and non-USA (including Canada, Netherlands, and Sweden) | RCT | Workplace "stay at work" and RTW interventions--defined by changes to the workplace or equipment, changes in work design and organization, changes in working conditions or environment, and occupational (case) management with active stakeholder involvement of (at least) the worker and employer--compared to "usual care" (no intervention) and clinical interventions | Employer | Working-age adults (ages 18-65) on work disability with LBP, upper extremity disorders, or musculoskeletal disorders at risk of leaving work because of sickness | The authors synthesized 6 RCTs. There is moderate quality evidence to support the use of workplace interventions to reduce sickness absence among the subgroup of workers with musculoskeletal disorders when compared to usual care. No convincing conclusions could be formulated about the effectiveness of workplace interventions on other work-related outcomes, regardless of work disability type. Considering all types of work disability together, the results showed low quality evidence that workplace interventions are more effective than usual care in reducing absence from work because of sickness. |
| Gensby et al. (2012), USA | RCT | WPDM programs promoting RTW | Employer | Workforce re-entering employees with injuries or illnesses (occupational or non-occupational) | There was a lack of evidence to draw conclusions about the effectiveness of employer-provided WPDM programs; thus, the review could not determine whether specific program components or specific sets of components are driving effectiveness. |
| Carroll et al. (2010); non-USA (Sweden, Netherlands, UK, and Canada) | Longitudinal and controlled | Interventions involving the workplace vs. those that do not; RTW | Employer | People, particularly those suffering from back pain and related musculoskeletal conditions, currently employed but at risk of job loss due to disability | Interventions involving employees, health practitioners, and employers in collaboration are more consistently effective than other interventions. EI was found to be effective. An economic evaluation indicates that interventions with a workplace component are likely to be more cost-effective than those without. |
| Cimera (2012); USA | Cost accounting | SE, broadly speaking | Employer/ community | Disabled persons who participate in SE programs vs. disabled persons who work in segregated settings/ workshops | Individuals with disabilities experience greater monetary benefits than costs when working in the community under conditions of SE. Cost efficiency appears to hold, regardless of type of disability and the presence of secondary conditions. Recent research strongly suggests that SE returns approximately $1.46 per dollar of taxpayers' cost. Literature suggests that SE is more cost-effective than sheltered workshops. This is the case whether cumulative costs, cost per hours worked, dollar earned, or months of service are compared. |
| Franche et al. (2005); USA | RCT, and QED and cohort design | Workplace-based RTW interventions and health care provider interventions | Employer | Working individuals with musculoskeletal disability or other pain-related condition, at risk of job loss | Workplace-based RTW interventions can reduce work disability duration and associated costs. Researchers found strong evidence that work disability duration is significantly reduced by work accommodation offers and contact between health care provider and workplace, as well as moderate evidence that it is reduced by interventions that include early contact with the worker by workplace, ergonomic worksite visits, and the presence of an RTW coordinator. For these 5 intervention components, there is moderate evidence that they reduce costs associated with work disability duration. Evidence for sustainability of these effects is limited. |
| Westbrook et al. (2012); USA and non-USA | QED; authors also reviewed qualitative studies | Competitive/ supported/ integrated employment assistance interventions, including job finding, work preparation, communication with employers, and job coaching | Employment-support workers; adult service program agencies | Unemployed adults 18 and older with ASD, not enrolled in a school-to-work or secondary-level education program, voluntarily trying to secure employment | A review of two QED studies was unable to identify definitive interventions that predictably and positively support the development of employment outcomes for individuals with ASD. Qualitative work suggested the following elements as promoting employment placement among people with ASD: identification of the most appropriate work settings and placements; provision of effective supports on-the-job; long-term support services for the employer and consumer; costs for support; positive effects of employment on persons with ASD. Qualitative studies could not, however, provide definitive statements about what works. |
| Williams et al. (2007); USA and non-USA (including Denmark, Germany, Israel, Sweden, and Netherlands) | Prospective; cross-sectional | Workplace rehabilitation interventions, including early RTW/ modified work interventions, ergonomics, and supervisor involvement | Employers and health care providers | Injured workers with musculoskeletal work-related LBP, trying to return to and/or at risk of leaving work | Evidence that clinical interventions combined with occupational interventions as well as early RTW/modified work interventions were effective in returning workers to work faster. Early RTW/modified work was effective in decreasing the rates of back injuries as well as lost-time back injuries, especially when accompanied by early contact with the worker by the workplace, and a health care provider intervention at the workplace. Ergonomic interventions--including exercises, lumbar supports, participatory ergonomics, and workplace adaptation--were also found effective in returning injured workers to work. |
| Tompa et al. (2008); USA and non-USA (Sweden, Finland, and Canada) | Economic analyses, the majority of which included a cost-benefit/cost-consequence analysis; analyses ranged in design from RCTs to uncontrolled experiments to pre-post | 17 DM interventions, including vocational and ergonomic interventions, standard care, behavior-oriented physiotherapy, and recovery/case management | Mix of employer financed and non-employer financed | Various disabilities | The review found strong evidence supporting the economic merits of DM interventions conducted in multiple industries. There is moderate evidence for interventions that include an education component, moderate evidence for those with physiotherapy, limited evidence for those with a behavioral component, and moderate evidence for those with a work/VR component. There is moderate evidence for interventions including a work accommodation offer, contact between the health care provider and workplace, early contact with the worker by workplace, ergonomic worksite visits, and interventions with an RTW coordinator. |
| Lounds-Taylor et al. (2012); USA and non-USA (including Spain, Germany, and UK) | QED, cohort studies, case series, and cross-sectional study | VR and interventions; on-the-job supports; community work and SE programs | Employers/ the community | Young adults ASDs | Little evidence is available for specific vocational treatment approaches as members of the population transition into adulthood. The majority of studies included, of which there were a limited number, suggest that vocational programs may increase employment success for some. |
| Khan and Stokes (2011); USA | RCT and non-RCT studies with comparison groups | VR vs. alternative programs or care as usual on return to work | Employer | Individuals with MS attempting to return to work | There is insufficient evidence for VR programs for: (a) "competitive employment" in altering rates of job retention, changes in employment, improvement in rates of re-entry into the labor force; and (b) altering "work ability" by improving participants' confidence in the accommodation request process or employability maturity or job-seeking activity. There is no evidence for changes in proportions of persons in SE or on disability pensions, or for cost-effectiveness. Inconclusive evidence to support VR for MS. |
| Dibben et al. (2012); USA and non-USA (including UK, Netherlands, Australia, and various Scandinavian countries) | Quantitative (RCT, QED, and small- scale studies) and qualitative research designs | Various health, work, and social interventions designed to help people with common health conditions stay in work or return to work, including workplace-based CBT, workplace-based patient education, VR, and encouragement of physical activity | Employer | People with common health conditions, either out of work or possibly at risk of job loss | The evidence base for work-related interventions for people with common health conditions has not changed substantially since 2007, and studies generally lack robust quantification of employment outcomes and cost/benefit analysis of interventions. Little quantitative evidence is available for interventions carried out in the UK. Areas in which there is a reasonably strong body of evidence, with positive effects, include the following: workplace-based interventions for those with musculoskeletal disorders, particularly for LBP; CBT, VR and workplace rehabilitation for LBP; SE for people with severe mental health conditions; and psychological interventions for depression. Some evidence of the benefits gained from coordination between rehabilitation professionals and the value of a case management approach among studies examining interventions for people with general health conditions. The majority of studies on musculoskeletal conditions focus on LBP, with some evidence that a multidisciplinary approach, including CBT and workplace-focused interventions, are effective in terms of benefits and costs. Evidence on other interventions is either of low quantity, poor quality, or inconclusive. |
| Livermore and Goodman (2009); USA | RCT and QED | Government initiatives involving work supports, One-Stop Centers, job training, case management, work incentives, work incentives counseling, and expanded options for ENs or rehabilitation services. Authors also examined legislation, policies, and tax incentive-based initiatives | Government | SSI/SSDI beneficiaries with various disabilities; individuals with severe/significant disabilities, including those with limited or no work experience | Among the findings reported, the most germane to this report include the following: TTW, a program for persons receiving SSDI, provided employment-support options and opportunities for participants. Enrollees could select a range of public or private EN services, including state-federal VR. TTW provided greater consumer choice than previous programs. Evaluations of TTW indicate the impact on earnings was too small to evaluate compared to historical trends. Based on evaluation report findings, each report author suggests similar components needed for an intervention to produce an impact on employment. |
| Wittenburg et al. (2008); USA | RCT and QED | Government demonstrations involving work supports, case management, job training, work incentives counseling, and expanded options for ENs or rehabilitation services | Government | SSI/SSDI beneficiaries with various disabilities | Among the findings reported, the most germane to this report are from the 1980s and include the following: The STETS T group had an employment rate 63% higher and earnings 74% higher than the C group. TETD, an employment-support program for individuals with intellectual disabilities, also reported a significant impact on employment rates and benefit amounts. After 6 years of enrollment, persons in the T group had earnings 56% greater than those not receiving the services. |
| Schandelmaier et al. (2012); USA and non-USA | RCT | RTW coordination involving direct assessment and individually tailored RTW, compared to usual practice in patients at risk for long-term disabilities. | Private disability insurance | Employees on sick absence for at least 4 weeks; primarily consisting of workers with musculoskeletal disorders and LBP | Overall, there was moderate evidence to suggest the benefit of RTW coordination on reduction in sick leave and returning to work. Authors note that publication bias could limit the results. |
| Clayton et al. (2011); non-USA (UK and others) | Observational studies | Interventions involving case management, personal advisors, job-search assistance, and financial incentives | Government | Individuals with disabilities who were not employed and on some form of incapacity-related benefit. | RTW interventions with components such as personal advisors and individual case management helped participants return to work. However, the review consisted primarily of observational studies. No RCTs were included in the review and there was evidence of selection bias in some of the programs; hence, there is limited evidence of effectiveness. |
| NOTE: Underlined studies indicate that the study reported statistically significant intervention-comparison differences for one or more outcomes. T=treatment (group); C=control (group). |
|||||
APPENDIX B: Methodology for the Literature Searches
In this appendix, we detail the methodology we employed to conduct two targeted literature searches: one on employment programs and outcomes for people with psychiatric disorders and one on employment programs and outcomes for people with other disabilities. The literature search and review process for both searches consisted of five stages: (1) systematically retrieving peer-reviewed literature; (2) sorting references; (3) identifying gray literature and other studies; (4) identifying studies for inclusion in the review; and (5) summarizing relevant articles.
A. Systematically Retrieving Peer-Reviewed Literature
We first developed a systematic information-retrieval plan. In consultation with a library information specialist, the chapter authors identified the suite of relevant databases and indexes to search: PubMed, PsychInfo, Cochrane Database of Systematic Reviews, Scopus, and CINAHL. Searching several databases minimizes the risk of selection bias from any one database. We narrowed the field to articles published in English in the last 20 years (1992-2012).
We then selected appropriate key word terminology for each subgroup and SE (Table A.1). We tailored the search terms to each database to allow for differences in terminology, search syntax, spellings, use of truncation, and organization and indexing of content. For the review of evidence on employment for people with psychiatric disorders, the search for each subgroup included general terms for: (1) disability type, including psychotic disorders, mental disorders, severe mental illness, and schizophrenia; and (2) employment terms, such as employment outcomes, employment supports, and work supports. To these key words we added language specific to each subgroup and retrieved the following:
-
Long-term users of mental health services. Additional key terms included specific target populations (veterans and homeless, for example) and disorders, (PTSD, for example). We retrieved 192 unduplicated articles.
-
Individuals at risk of job loss. Additional key words included likely employment-support programs (employer disability insurance, employee assistance programs, VR, and reasonable accommodation, for example). We retrieved more than 600 unduplicated articles.
-
Individuals experiencing an FE of psychosis and TAY. Due to the overlap in terminology, we combined the database searches for these two subgroups. Language to isolate the populations included FE, young adults, onset of psychosis, and youth in transition. We retrieved 64 unduplicated articles.
-
SE. Given the specificity of this topic and the extensive literature base, we restricted the search terms to SE, systematic reviews, and reviews. We retrieved 112 unduplicated articles.
For the review of evidence on employment supports for people with other disabilities, we searched for and summarized existing systematic reviews and meta-analyses concerning services and supports designed to increase employment among people with disabilities. We excluded employment interventions for people with mental disorders, as our previous literature review covered employment-support programs for this population. In addition to the databases mentioned above, we searched Campbell Collaboration, AHRQ, Academic Search Premier, SocINDEX, EconLit, the National Center for the Dissemination of Disability Research Registry of Systematic Reviews, and Business Source Corporate.29 Keywords and phrases developed for the searches were assigned to four groups and truncated if necessary (Table A.1). The searches yielded 221 potentially relevant studies.
B. Sorting Peer-Reviewed Literature
We stored reference information for articles retrieved through this process in RefWorks, an online reference-management application. In RefWorks, we reviewed article titles, authors, and abstracts to sort through the unduplicated studies by subgroup. Studies were excluded that: (1) focused on a disability group other than psychiatric disorder, or focused on the disability population as a whole; (2) did not focus on employment; (3) did not report on study results (such as opinion pieces). Remaining articles were sorted by study design: systematic review, non-systematic review, RCT, quasi-experimental design (QED), pre-post design, implementation study, and "other."
For the review of evidence on employment programs for people with other disabilities, two reviewers independently examined systematic review titles and abstracts related to disability, RTW, DM, and employment outcomes. We excluded summaries of disability laws and policies, such as the ADA and Medicaid Buy-In, which do not include employment or RTW services at the individual or employer levels. We also excluded tax incentives for businesses to hire persons with disabilities. We also obtained relevant reviews and reports through Mathematica's subscription service and assessed them for inclusion. For each review or report included, we extracted pertinent information about the study types, design, key findings, and strength of the evidence reported (Table A.8). Those retained for screening met the following four criteria, as determined through independent examination of their titles and abstracts by two reviewers:
-
They did not focus on populations consisting solely of individuals with mental disorders.
-
They could be classified as systematic reviews, reviews, or meta-analyses.
-
They did not focus on medical/clinical interventions, unless these interventions were combined with employment services or supports.
-
They were published between January 1992 and October 2012.
C. Identifying Gray Literature and Additional Peer-Reviewed Studies
In addition to conducting an up-front, systematic search for peer-reviewed literature, we searched for gray literature and other suitable studies on a continuous basis by: (1) obtaining articles and reports of demonstration and research projects known to the authors, such as reports based on EIDP and TTW; (2) scanning the references of published articles identified above; and (3) searching websites of relevant government agencies, such as SAMHSA, the National Institute on Disability and Rehabilitation Research, and HHS, and research centers, such as the Rehabilitation Research and Training Centers on youth transition. In some instances, we contacted study authors to obtain unpublished articles or data, or published articles we could not locate.
Our initial scan did not identify published systematic reviews on workplace interventions for veterans or reviews that included national demonstrations for Social Security disability beneficiaries. To address this issue, we also included four reports that describe research on Social Security RTW demonstrations and Veterans Health Administration programs.
D. Identify Studies for Inclusion in the Review
We used a tiered-inclusion process to prioritize the most rigorous research available for each study group. We first selected systematic literature reviews to focus on the most rigorous research and take advantage of work already completed, then included RCTs, QEDs, and pre-post test designs. Our inclusion criteria for each subgroup varied according to the rigor of the literature base. For example, given the robust literature on SE, we primarily included systematic reviews, whereas for the newer area of FE research, we included a mix of RCTs, QEDs, and pre-post test designs. The number of studies included in the review is shown in the right column of Table A.1.
The review on evidence of employment programs for people with other disabilities included only systematic reviews. The review team double-checked each other's decisions about whether each study met the criteria listed above. If both agreed that the criteria were fulfilled, a librarian obtained the study's full text. Full-text articles underwent further assessment for inclusion, based on the germaneness of their subject matter. Reviews were included if they centered primarily on employment supports and services for people with physical, sensory, developmental, or intellectual disabilities, and if the outcomes of interest included employment. We included 15 studies in the review.
E. Summarizing Relevant Articles
After identifying articles for inclusion, we summarized each one in separate tables for each study group in order to consistently track key information. Each table included study identifiers, study description, research methodology, study population, sample size, results, and limitations. Simplified versions of these tables appear in Appendix A.
| TABLE B.1. Results of Literature Review | |||
|---|---|---|---|
| Area of Population Subgroup |
Search Terms | Number of Unduplicated Articles Identified |
Number of Articles Included* |
| SE | Supported employment; systematic reviews; reviews | 112 | 22 |
| Long-term users of mental health services | Serious mental illness; schizophrenia; bipolar disorder; psychiatric disability; post-traumatic stress disorder; depression; employment outcomes; vocational outcomes; job outcomes; work supports; employment supports; job supports; disability supports; vocational services; employment services; disability services; Social Security Disability Insurance; Supplemental Security Income; veterans; military; Temporary Assistance for Needy Families (TANF); homeless; criminal justice; immigrants; economic recession | 192 | 6,516 |
| Risk of job loss | Employer disability insurance; employee assistance programs; mental health parity; reasonable accommodations; job retention; job tenure; job support; depression; workplace; risk of job loss; mental health friendly workplace; return to work; employment outcomes; supported employment; vocational rehabilitation; mental disorders | >600 | 13 |
| FE/TAY | First episode; onset of psychosis; onset of schizophrenia; adolescents; young adults; youth in transition; psychotic disorders; mental disorders; serious emotional disturbances; supported employment; job support; employment outcomes; employment supports; work supports; individual placement; vocational rehabilitation; wrap-around services | 64 | 9 in FE section 5 in TAY section |
| Other employment supports | Articles were referred from research results on the above populations | 13 | 13 |
| Employment programs for people with other disabilities | Employment services/supports; disability management; vocational rehabilitation; Veterans Administration; impairment; blind; deaf; physical disability; intellectual disability; Supplemental Security Income; Social Security Disability Insurance; Medicaid; private disability insurance; systematic review; meta-analysis; review | 221 | 15 |
| NOTE: Studies on which evidence of the effectiveness of specific interventions is based. Excludes articles used for background material. This number includes articles identified through other sources, such as reference lists of literature reviews or reports. | |||
APPENDIX C: Data and Methodology for the SIPP Analysis
For this analysis, we pooled the 1996, 2001, and 2004 panels of the SIPP, a nationally representative sample of the non-institutionalized civilian population who are 15 years old and older. SIPP respondents are interviewed once every four months for the duration of the survey panel. During each interview, they provide information about the preceding four months. Each interview constitutes a wave; linking a series of waves creates a panel of 2-4 years. SIPP contains information on demographic characteristics, employment outcomes, and program participation of each respondent. A respondent's disability status can be identified in two ways. First, each SIPP wave asks respondents if they have a work limitation, which constitutes a work disability. Second, a topical module, asked at varying time points, asks respondents a series of questions regarding their disability and limitation status. We used the first approach to identify members with disabilities of various at-risk groups.
We linked SIPP data to SSA administrative files to identify SSDI application dates, SSDI receipt, and SSI receipt. Not all SIPP records could be matched to SSA administrative data, either because SIPP respondents did not provide Social Security Numbers (SSN), respondents opted out of having their data matched to federal records (beginning in 2004), or the information from the SIPP (SSN, name, gender, date of birth) did not match SSA administrative data (McNabb et al. 2009). The match rate for the panels is 84 percent for the 1996 panel, 60 percent for the 2001 panel, and 79 percent for the 2004 panel. The statistics presented here, therefore, represent lower-bound estimates and could potentially be biased if non-matched respondents systematically differ by SSDI receipt or application status from matched respondents. Using the SSA administrative data, we excluded individuals who received SSDI benefits as of the first SIPP wave from our analysis sample, tracked SSI receipt throughout the SIPP observation period (a more accurate approach than using the SIPP self-report data), and identified the earliest occurrence of a SSDI application up to six years after the first SIPP wave.
The sample for this analysis was restricted to those between the ages of 25 and 55 whose first survey response occurred in wave 1. We excluded individuals younger than age 25 because they are less likely to qualify for SSDI and more likely to be enrolled in school. We excluded individuals older than 55 because we wanted to avoid tracking individuals who could qualify for early retirement benefits during our six-year observation period.
We divided our analysis sample into the following groups of individuals considered to be at risk of applying for and receiving SSDI, and whom we term "at-risk group members:" unemployment benefit recipients with a disability, individuals with high health expenditures, workers' compensation beneficiaries, private disability insurance beneficiaries, veterans beneficiaries with a disability, and individuals with disabilities who have received job training or education services within the past year (see Table IV.1). We also included another group, workers with disabilities at risk of applying for unemployment benefits, whom we identified using a logistic regression model to predict the likelihood of unemployment benefit receipt; we selected individuals in the upper one-third of scores for this group.
We examined various characteristics for each analytical group. These characteristics include demographic variables (age, gender, race, marital status, and educational attainment), as well as specific employment, income, and program-participation measures (as defined in Table IV.2).
The analytical methods incorporated descriptive statistics, measured at a point in time or across six-month intervals, and comparative statistics (t-tests) to determine statistical significance. To improve the precision of our estimates, we show data only for statistics with at least 50 observations. Data are weighted using the SIPP panel wave 1 weights.
APPENDIX D: Supplemental Tables for Pre-Application Work Activity and Program Participation of SSDI Applicants and At-Risk Group Members
| TABLE D.1. Employment and Income Characteristics of SSDI Applicants | ||||||||
|---|---|---|---|---|---|---|---|---|
| 37-42 Months Before SSDI Application |
31-36 Months Before SSDI Application |
25-30 Months Before SSDI Application |
19-24 Months Before SSDI Application |
13-18 Months Before SSDI Application |
7-12 Months Before SSDI Application |
1-6 Months Before SSDI Application |
All Individuals Ages 25-55 |
|
| Labor force participation | ||||||||
| Any employment | 88.5% | 87.5% | 83.6% | 81.0% | 79.0% | 76.7%* | 66.4%** | 84.0% |
| Without a job/not looking for work | 17.9% | 20.2% | 23.4% | 24.9% | 29.1% | 34.6%* | 54.1%** | 16.7% |
| Monthly income (mean) | ||||||||
| Individual earned income | $1,887 | $1,865 | $1,656 | $1,531 | $1,507 | $1,356 * | $944** | $2,727 |
| Individual earned income of those with earnings | $2,364 | $2,309 | $2,204 | $2,080 | $2,151 | $2,082 | $1,941 | $3,399 |
| Individual total income | $2,068 | $2,071 | $1,860 | $1,766 | $1,767 | $1,699 | $1,396* | $2,892 |
| Household total income | $3,923 | $4,351 | $4,047 | $3,889 | $3,776 | $3,637 | $3,359 | $5,783 |
| Households under the FPL | 24.0% | 22.4% | 25.8% | 25.9% | 29.1% | 33.0% | 40.4%* | 13.4% |
| Unweighted Sample Size | 204 | 376 | 626 | 856 | 1,045 | 1,202 | 1,335 | 127,972 |
| Unweighted Sample Size (for individual earned income of those with earnings) | 183 | 323 | 515 | 689 | 822 | 904 | 841 | 104,834 |
| Weighted Sample Size (per panel) | 173,487 | 322,895 | 556,766 | 762,919 | 939,560 | 1,094,278 | 1,219,322 | 121,410,365 |
| SOURCE: 1996, 2001, and 2004 SIPP Panels matched to SSA administrative data. NOTES: Table shows employment and income characteristics of SSDI applicants in 6 month intervals before they applied for benefits. Income statistics adjusted to 2004 dollars using the Consumer Price Index for All Urban Consumers. The statistics for "individuals ages 25-55" are for individuals ages 25-55 in wave 1 of each panel, regardless of disability, SSDI, or at-risk group status. Statistics for each six month period were compared to the 37-42 month period using t-tests. * p<0.05 ** p<0.01 |
||||||||
| TABLE D.2. Sample Sizes of SSDI Applicants and Non-Applicants by At-Risk Group | ||||||
|---|---|---|---|---|---|---|
| At-Risk Group | 1-6 Months |
7-12 Months |
13-18 Months |
19-24 Months |
25-30 Months |
31-36 Months |
| Sample Sizes of Those Who Eventually Applied for SSDI Benefits | ||||||
| High health expenditures | 243 | 226 | 177 | 132 | 100 | 98 |
| Private disability insurance | 144 | 107 | 87 | ND | ND | ND |
| Job training | 112 | 108 | 105 | 79 | 50 | 52 |
| Unemployment insurance | 66 | ND | ND | ND | ND | ND |
| At risk of unemployment insurance | 108 | 105 | 106 | 105 | 80 | ND |
| Veterans | 158 | 141 | 136 | 118 | 103 | 55 |
| Workers compensation | 139 | 110 | 96 | 52 | ND | ND |
| Sample Sizes of Those Who Did Not Apply for SSDI Benefits | ||||||
| High health expenditures | 3,882 | 3,717 | 2,945 | 2,429 | 1,512 | 1,482 |
| Private disability insurance | 518 | 355 | 287 | 167 | 105 | 52 |
| Job training | 1,091 | 1,043 | 974 | 783 | 465 | 459 |
| Unemployment insurance | 386 | 304 | 240 | 159 | 96 | 63 |
| At risk of unemployment insurance | 602 | 592 | 593 | 589 | 457 | 232 |
| Veterans | 942 | 816 | 793 | 697 | 582 | 187 |
| Workers compensation | 863 | 597 | 503 | 301 | 238 | 136 |
| Weighted Sample Sizes of Those Who Eventually Applied for SSDI Benefits | ||||||
| High health expenditures | 220,372 | 205,284 | 163,849 | 131,911 | 90,020 | 88,121 |
| Private disability insurance | 137,694 | 100,836 | 82,093 | 48,125 | 28,477 | 16,938 |
| Job training | 104,142 | 100,333 | 98,564 | 74,429 | 46,830 | 48,070 |
| Unemployment insurance | 59,211 | 41,995 | 37,201 | 23,801 | 12,562 | --- |
| At risk of unemployment insurance | 99,095 | 97,045 | 97,562 | 96,487 | 73,686 | 40,801 |
| Veterans | 147,701 | 133,957 | 126,294 | 108,698 | 94,048 | 47,158 |
| Workers compensation | 134,044 | 105,919 | 93,904 | 50,214 | 41,047 | 18,887 |
| Weighted Sample Sizes of Those Who Did Not Apply for SSDI Benefits | ||||||
| High health expenditures | 3,652,961 | 3,512,435 | 2,804,660 | 2,396,035 | 1,410,873 | 1,379,665 |
| Private disability insurance | 489,434 | 334,756 | 269,773 | 157,516 | 98,966 | 48,391 |
| Job training | 1,008,617 | 966,632 | 906,395 | 727,057 | 433,145 | 429,627 |
| Unemployment insurance | 362,740 | 287,047 | 221,496 | 149,390 | 91,058 | 60,456 |
| At risk of unemployment insurance | 572,114 | 561,501 | 562,782 | 558,806 | 441,362 | 209,691 |
| Veterans | 871,554 | 754,836 | 733,463 | 643,983 | 535,054 | 174,820 |
| Workers compensation | 813,651 | 554,886 | 466,114 | 276,535 | 220,885 | 124,335 |
| SOURCE: 1996, 2001, and 2004 SIPP Panels matched to SSA administrative data. NOTES: Table shows number and weighted number of at-risk group members across all three panels at six month intervals after they were identified in the at risk group. ND=no data (sample size less than 50 across all three panels). |
||||||